


Comprehensive Compression Therapy for the Lower Extremities
Compression therapy remains the gold standard for managing lower extremity edema, yet its application is often underutilized due to clinical uncertainty. Understanding the edema continuum—and how patients move along it—is essential to selecting the right compression modality at the right time. This comprehensive review breaks down therapy types, indications, and practical guidelines to support confident, evidence-based care.
Key Takeaways
1. Edema exists on a continuum driven by lymphatic dysfunction.
All forms of peripheral edema, whether acute or chronic, reflect some degree of lymphatic impairment. Recognizing where a patient falls on this continuum is critical to tailoring compression therapy and adjusting treatment as conditions evolve.
2. Compression is not one-size-fits-all; modality and dosage matter.
From static to dynamic systems, each option delivers different pressure profiles and clinical benefits. Appropriate selection depends on etiology, severity, tissue quality, and patient mobility; similar to prescribing the correct medication and dose.
3. Safe and effective compression requires proper assessment and training.
Vascular screening, awareness of contraindications, and patient-specific factors are essential before initiating therapy. Clinician education in both selection and application techniques is key to improving outcomes and reducing underuse.
Compression therapy is the gold standard for peripheral edema management. That is not a new or bold statement, but to understand the multiple compression options, guidelines, restrictions, and techniques in applying appropriate compression, we must first identify the peripheral edema continuum. Edema is the accumulation of extraneous fluid in the intercellular tissue spaces, resulting from a disrupted capillary exchange where the filtration exceeds lymphatic drainage. Hettrick and Aviles1 posited that all edema, whether it is a transient or chronic fluid overload, is a version of lymphatic dysregulation, and essentially all edema is some form of lymphedema on a continuum. That lymphatic dysregulation can occur when the lymphatic vessels or nodes cannot properly drain and can result from primary conditions such as genetic mutations of the blood vessels, as well as a variety of secondary conditions such as surgeries, traumas, cancer treatments, infections and parasites, and chronic diseases such as congestive heart failure and venous insufficiency.2
Regardless of the originating cause, the resultant dysfunction of the lymphatic system can lead to skin changes, delayed wound healing, chronic, painful swelling to limbs and digits, feelings of heaviness and tightness to extremities, and restricted range of motion. In practice, there is often suboptimal utilization of compression therapy because of confusion and lack of confidence as to when and how to use it. Understanding the edema continuum and how a patient may fluctuate along that continuum can guide a clinician in choosing the right compression therapy for the right patient at the right time.
More than Edema Control: The Therapeutic Benefits of Compression
Appropriate compression management can address many issues besides the obvious reduction of swelling. It can help with pain, protected range of motion, as well improve skin quality to assist in wound healing. It can assist with short-term peripheral decongestion as well as long term management of healing by releasing inflammatory and vasoactive mediators. The central goals of adequate compression management are to:
- improve hemodynamics by increasing fluid movement through the venous and lymphatic system;
- support tissue structure by reducing skin tension; and
- improve pain and immune function by reducing metabolic waste accumulation.
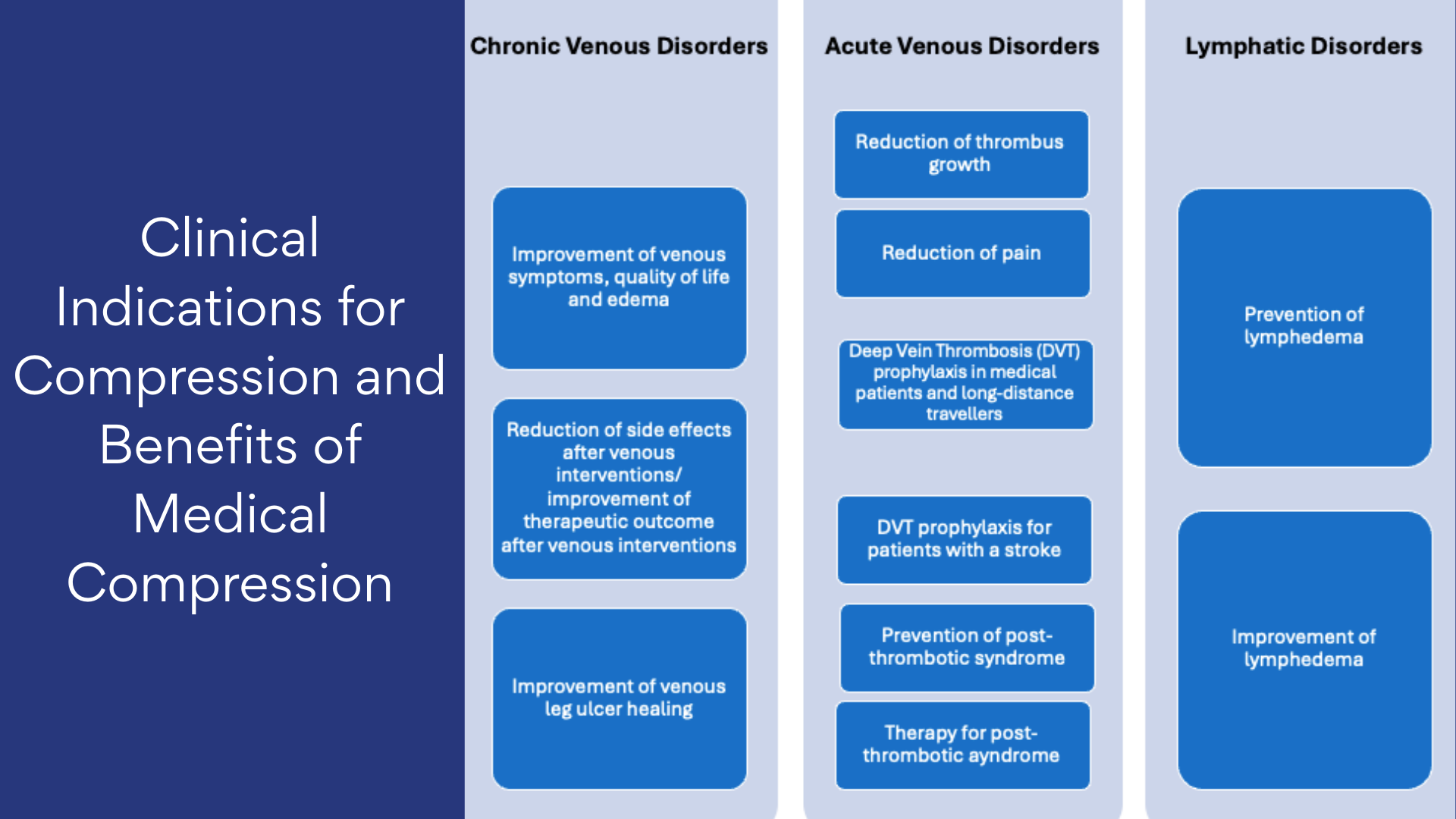
Who Benefits from Compression? Clinical Indications Explained
In their 2008 position paper on medical grade compression, the International Compression Club (ICC) recommended using compression therapy to manage venous and lymphatic diseases, including lymphedema, lipedema, and phlebolymphedema.4 Rabe and colleagues further posited that because compression has an anti-inflammatory effect, it is recommended for inflammatory conditions that also have an edema component. This can include cellulitis, vasculitis, and other systemic medical treatments.5 Compression therapy has also been shown to be safe and effective in addressing lower extremity edema and improving mobility in patients with stable chronic heart failure (CHF), particularly for those that fall under stable New York Heart Association (NYHA) Class II or III.6 Management of edema should be guided by the also addressing the underlying etiology. Prescribing appropriate compression therapy should be approached in the same manner as prescribing appropriate medication types, dosage, and timing for each specific patient pathology. Application of appropriate compression therapy is a skill that needs to be taught taught just as widely as we teach suturing techniques.
Compression Therapy Methods: Static Versus Dynamic
Static compression therapy utilizes a constant level of pressure with the use of garments or bandages. Within each type of static compression, there are options for different levels of compression. Dynamic compression utilizes intermittent pneumatic pumps and actively forces fluid out of the limb by mimicking muscle pumps. Different compression dosage levels and programs can also be set depending on the patient’s swelling patterns and amount of skin changes.
Static Compression Options
- Elastic and long stretch bandages: Generally, stretchable, breathable wraps that have high elasticity and high recoil. An example of these is an ACE wrap. Long-stretch bandages provide high resting pressure but have a lower working pressure. The fibers allow for the bandage to stretch as edema increases, which is generally not recommended to be used alone when treating venous insufficiency or lymphedema. These are generally recommended for acute sprains and strains or for securing bandages and are suitable for mobile patients that require continuous pressure during movement.7
- Inelastic and short stretch bandages: Short-stretch bandages are composed of nonelastic/inelastic or more rigid materials with elasticity ranging from 20% to 90%. They typically exert higher working pressures compared to long-stretch bandages, with lower resting pressure. Zinc-paste bandages (such as Unna’s boots) are limited in their efficacy in the early decongestion phase while there is still significant volumetric instability. Compression develops as the paste dries to form a somewhat inelastic mold with low resting pressure and higher working pressure while a patient ambulates. Short stretch bandages are generally recommended over long stretch due to the ability to stabilize tissue hydrostatic pressure and improve venous and lymphatic flow.7
- Multilayer compression bandage systems: These systems will usually consist of 2-4 layers of bandaging with padding, light support, compression, and cohesive bandages. Depending on the system, different final pressures and gradients may result that are also dependent on postural changes.8 These are generally recommended for venous ulcerations.
- Multicomponent bandage systems: Multicomponent systems are generally ready-made 2-layer bandage systems with both short and long stretch bandages. These systems provide high working pressure and low resting pressure. Because these systems tend to be less bulky than their multi-layer compression counterparts, they tend to be well tolerated by patients.9

- Compression stockings/garments: Both ready-to-wear and custom compression stockings offer an easy solution for patients. They bracket both ends of the continuum in that they provide a first-line therapeutic option for edema as well as a long-term maintenance solution for when the patient is volumetrically stable. The effectiveness of the compression stocking is dependent on the dose (mmHg), and the elasticity and stiffness of the textile used. When prescribing compression stockings, patient mobility, skin texture, quality of edema, as well as swelling patterns and location can guide whether management is best with a ready-to-wear versus a custom-made compression stocking.10
- Circular Knit Garments: Circular knit garments are generally ready-to-wear but can be customized. The yarn tends to be finer and the garment is overall less stiff. Circular knit stockings tend to be adequate for early venous disease without significant shape distortion due to edema.
- Flat Knit Garments: Flat knit garments can be either ready-to-wear or custom-made and are generally for patients who have volumetrically stable edema, but may have additional shape distortion. The yarn tends to be thicker and stiffer, which creates more wall stability and less stretch over time. The garments are usually made of flat sheets knitted together, which allow bridging over skin folds and avoids a tourniquet effect over skin folds when customized to irregularly shaped limbs.10
- Night Garments—Night garments can actually be worn at night or during the day. Their main function is to prevent rebound swelling as well soften fibrotic skin changes associated with edema. Adding different foam pieces into the garment can more focally address keratotic and fibrotic areas. Prescribing this type of garment usually takes place after decongestive therapy once the patient is volumetrically stable.


- Decongestive Garments—Decongestive garments are adjustable and customizable wraps ordered during the initial or acute decongestive phase of lymphedema therapy. They are generally stiffer in construction and have high working pressure and low resting pressure.

- Static pneumatic gradient compression: This is a new type of removable, wearable, inelastic compression device that offers adjustable compression with the use of a hand pump and air pressure gauges. With the built-in gauges, one can monitor and adjust compression level consistently throughout the day. It is a hybrid of both static and dynamic compression therapy, recommended for patients with lymphedema and chronic venous insufficiency.11

Dynamic Compression Options
- Intermittent pneumatic compression: Intermittent pneumatic compression therapy refers to any device using air to provide compression. These devices work to improve venous circulation, enhance arterial blood flow, and increase lymphatic system function to evacuate and redirect edema fluid.12,13 Within this category are sequential compression devices, which sequentially inflate with air from distal to proximal. Forced inflation and deflation of air bladders in a sequential manner mimics the limb’s vasculature during muscle contraction. The treatments are generally targeted for patients with chronic venous insufficiency, venous stasis ulcers, and lymphedema.
- Nonpneumatic Active Compression Device: These are wearable compression garments that deliver active sequential gradient compression with muscle pump activation while the patient can remain mobile. This occurs through a programmable segmental controller that contracts and relaxes a flexible frame within the garment. This is recommended for those with lymphedema, chronic venous insufficiency, and venous wounds.
Compression Therapy Guidelines to Consider
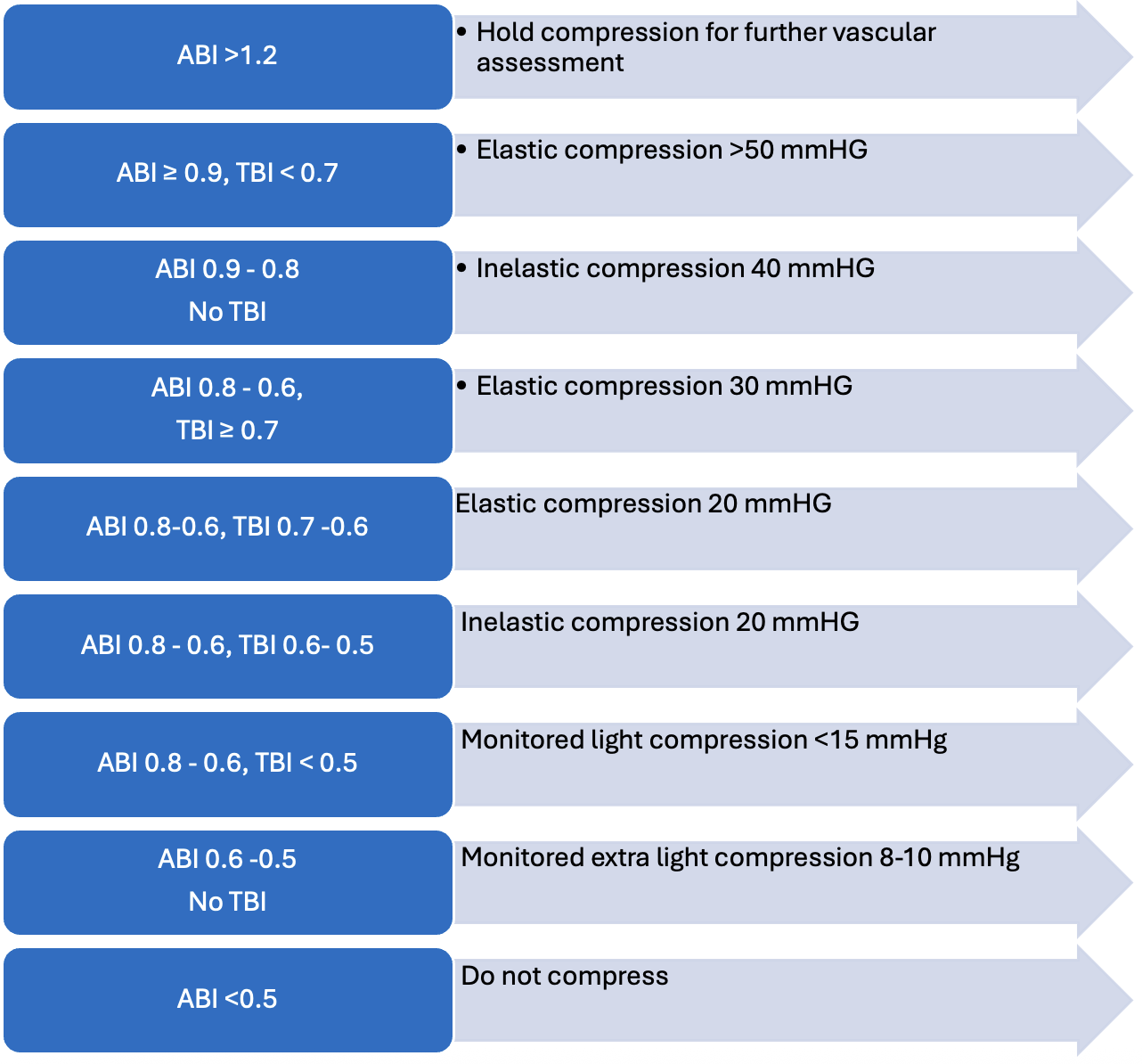
Before determining appropriate and safe compression options, a physical exam and vascular assessment should rule out significant arterial disease. For best practices, one should obtain an ankle-brachial index (ABI) and/or toe-brachial index (TBI). An ABI above 0.9 is generally safe for higher compression levels. An ABI above 1.2 requires additional vascular testing due to the higher level being indicative of noncompressible arteries and small vessel disease. Below 0.9 requires additional vascular testing to evaluate for mixed venous and arterial disease. In general, it is not recommended to compress below an ABI of 0.5. Further recommendations for compression therapy when combining information for both ABI and TBI are listed in Table 2.14,15
Besides an ABI < 0.5, other contraindications of compression can include ischemic pain, untreated deep vein thrombosis, untreated wound infection, and uncompensated organ failure (heart, lung, or renal). Precautionary monitoring of compression should also be taken in patients with cognitive decline or who are at high fall risk.15
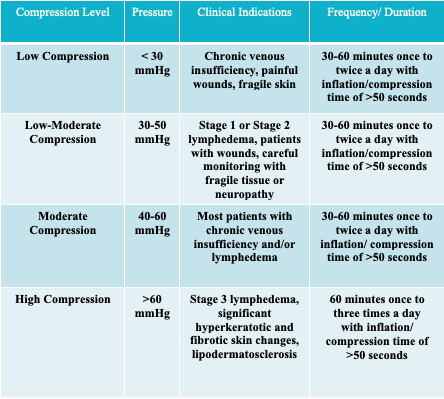
For intermittent compression therapy, the recommended compression dosage and timing for clinical indications is outlined in Table 3. The higher the dosage of compression, the more it will address fibrotic skin changes. Conversely, for patients with fragile tissue, recommendations outline starting the compression at a lower dosage.16,17
Lymphedema Treatment Act
It would be remiss not to mention the Lymphedema Treatment Act (LTA), effective January 1, 2024, in this comprehensive review of lower extremity compression therapy. The LTA is a federal law that amends Medicare to provide coverage of prescribed compression garments and bandages to lymphedema patients.18 Prior to the passing of the LTA, Medicare did not cover these essential and sometimes costly items to patients with lymphedema. LTA established a standard for Medicare and private insurers to cover lymphedema garments. It typically covers up to 3 daytime ready-to-wear or custom fit garments per affected body part as well as wraps, bandaging systems, and donning and doffing accessories every 6 months. It also covers 2 nighttime garments per affected body part every 2 years.18
Conclusion
Edema occurs along a continuum. It may be temporary or chronic. Understanding where a patient initially presents along that continuum and adjusting as the edema worsens or improves is essential to prescribing compression appropriately. Compression is the gold standard for managing edema, however, not all compression is equal, and it is important to recognize the many categories as well as levels of compression for safe and successful therapy.
Dr. Loan Lam is the Medical Director of Wound Services at United Vein and Vascular Centers. She is board certified in wound care, lymphedema, and hyperbaric medicine. She serves on the board of the Save a Leg, Save a Life Foundation.
References
- Hettrick H, Aviles F Jr. All edema is lymphedema: progressing lymphedema and wound management to an integrated model of care. Wounds. 2022;68(1):8-15.
- Yuan Y, Arcucci V, Levy SM, Achen MG. Modulation of immunity by lymphatic dysfunction in lymphedema. Front Immunol. 2019;10:76. doi:10.3389/fimmu.2019.00076
- Liao S, Padera TP. Lymphatic function and immune regulation in health and disease. Lymphat Res Biol. 2013;11(3):136-143. doi:10.1089/lrb.2013.0012
- Partsch H, Flour M, Smith PC, et al. Indications for compression therapy in venous and lymphatic disease: consensus based on experimental data and scientific evidence. Int Angiol. 2008;27(3):193-219.
- Rabe E, Partsch H, Hafner J, et al. Indications for medical compression stockings in venous and lymphatic disorders: an evidence-based consensus statement. Phlebology. 2018;33(3):163-184. doi:10.1177/0268355516689631
- Urbanek T, Juśko M, Kuczmik WB. Compression therapy for leg oedema in patients with heart failure. ESC Heart Fail. 2020;7(5):2012-2020. doi:10.1002/ehf2.12848
- Vowden P, Kerr A, Mosti G. Demystifying mild, moderate and high compression systems—when and how to introduce “lighter” compression. Wounds International. Published 2020. Accessed March 23, 2026. https://www.woundsinternational.com
- Dale JJ, Ruckley CV, Gibson B, Brown D, Lee AJ, Prescott RJ. Multi-layer compression: comparison of four different four-layer bandage systems applied to the leg. Eur J Vasc Endovasc Surg. 2004;27(1):94-99. doi:10.1016/j.ejvs.2003.10.014
- Stücker M, Münter KC, Erfurt-Berge C, et al. Multicomponent compression system use in patients with chronic venous insufficiency: a real-life prospective study. J Wound Care. 2021;30(5):400-412. doi:10.12968/jowc.2021.30.5.400
- Bjork R, Ehmann S. S.T.R.I.D.E. professional guide to compression garment selection for the lower extremity. J Wound Care. 2019;28(Suppl 6a):S1-S44. doi:10.12968/jowc.2019.28.Sup6a.S1
- Mosti G, Gasparis A, Oropallo A, Labropoulos N. Pressure and stiffness of a new air-inflated compression wrap. Phlebology. 2024;39(7):456-464. doi:10.1177/02683555241246606
- Zaleska M, Olszewski WL, Cakala M, et al. Intermittent pneumatic compression enhances formation of edema tissue fluid channels in lymphedema of lower limbs. Lymphat Res Biol. 2015;13(2):146-153. doi:10.1089/lrb.2014.0010
- Janßen S, Schmölders J, Jansen TM, et al. Intermittent pneumatic impulse compression in the treatment of stasis dermatitis—a monocenter randomized controlled trial. J Clin Med. 2025;14(10):3321. doi:10.3390/jcm14103321
- Elhomsy S, Chrusciel J, Sanchez S, et al. Clinical efficacy and safety of long-term compression in patients with mixed arterial and venous etiology ulcers in the leg. Int J Angiol. 2021;31(1):34-39. doi:10.1055/s-0041-1735204
- Weller CD, Team V, Ivory JD, et al. ABPI reporting and compression recommendations in global clinical practice guidelines on venous leg ulcer management: a scoping review. Int Wound J. 2019;16(2):406-419. doi:10.1111/iwj.13048
- Zaleska M, Olszewski WL, Jain P, et al. Pressures and timing of intermittent pneumatic compression devices for efficient tissue fluid and lymph flow in limbs with lymphedema. Lymphat Res Biol. 2013;11(4):227-232. doi:10.1089/lrb.2013.0016
- Partsch H. Compression therapy: clinical and experimental evidence. Ann Vasc Dis. 2012;5(4):416-422. doi:10.3400/avd.ra.12.00068
- Lymphedema Advocacy Group. Final LTA Rule. Published August 2024. Accessed March 23, 2026. https://lymphedemaadvocacygroup.org/wp-content/uploads/2024/08/Final-LTA-Rule-.pdf
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.





