

Through the Payer Lens: Real‑World Evidence That Changes Access
As regulators and payers place growing emphasis on real-world evidence, new survey findings reveal what managed care decision-makers value most—and how manufacturers can generate and communicate evidence that meaningfully influences coverage and formulary decisions.
Introduction
Regulatory Momentum and Payer Demand Have Made Real-World Evidence More Consequential for Coverage and Formulary Decisions
The United States Food and Drug Administration (US FDA) has maintained a long-standing commitment to real-world data and real-world evidence (RWE), using both to monitor postmarket safety and, with growing frequency, to inform effectiveness determinations.1 The 21st Century Cures Act of 2016 accelerated that trajectory, prompting the FDA in 2018 to establish a formal framework for evaluating how RWE might support new indications for already approved drugs or satisfy postapproval study requirements.1 Since 2011, the FDA’s Center for Drug Evaluation and Research and Center for Biologics Evaluation and Research have applied RWE across product approvals, labeling changes, and safety assessments, with 35 drugs, biologics, or vaccines, and more than 250 device authorizations incorporating RWE in their applications since 2016.2,3 In December 2025, the agency removed a consequential barrier: the prior requirement that marketing submissions always include identifiable individual patient data from real-world sources.3 That policy shift opens the door to de-identified datasets, including national cancer registries, insurance claims databases, hospital system records, and electronic health records— systems that had previously been impractical for submission purposes.3
On the payer side, parallel developments are sharpening expectations. The Academy of Managed Care Pharmacy published its first payer-specific RWE standards in December 2025, consisting of a product life cycle framework and a 29-criteria assessment checklist designed to guide both evidence generation and payer evaluation.4 That initiative found broad interest among managed care decision-makers in incorporating RWE into formulary and coverage processes, alongside a recognition that structured standards and targeted education were needed before routine adoption could occur.4 Taken together, these regulatory and payer-facing developments create a different operating environment for manufacturers. RWE is no longer a peripheral evidence stream assembled after launch and presented loosely; it is an expected input to coverage decisions, and organizations best positioned to gain traction are those that plan evidence early, tie it to specific payer questions, and present it in a clear, transparent structure that directly informs access decisions.
To better understand how payers are currently evaluating and applying RWE, Precision AQ conducted a national survey of managed care decision-makers in Q4 2025.
Survey Methodology
Participants were recruited from a proprietary database developed and owned by Precision AQ, comprising more than 6000 health care decision-makers. The survey was fielded using the Qualtrics platform and consisted of 10 multiple-choice questions. The research objectives were to assess the role of RWE in influencing coverage decisions, identify the therapeutic areas in which RWE will have the greatest impact, learn which types of RWE are most impactful to payers, and identify the greatest challenges payers face with using RWE.
The respondent base included 25 payer decision-makers representing eight national health plans, 10 regional health plans, and seven pharmacy benefit managers (PBMs). The sample comprised 9 medical directors and 16 pharmacy directors.
The Therapeutic Areas Where RWE Is Most Important to Payers
RWE Is Needed in Therapeutic Areas Where Payer Uncertainty, Budget Pressure, and Clinical Complexity Converge
Metabolic conditions, including diabetes, ranked as the top therapeutic area of interest, with 64% of respondents identifying it as a priority for RWE over the next 12 months (Figure 1). Oncology and hematology followed at 60%, whereas inflammatory and immunologic conditions and rare disease each registered at 56%. Cardiovascular conditions drew 28%, respiratory 16%, and neurology 8%. The concentration at the top of this list maps directly to categories where plan-level budget pressure, utilization management complexity, and unresolved clinical questions are most acute. The heightened interest in diabetes and metabolic disease is likely connected to the rising costs and broad use of glucagon-like peptide-1 (GLP-1) therapies.
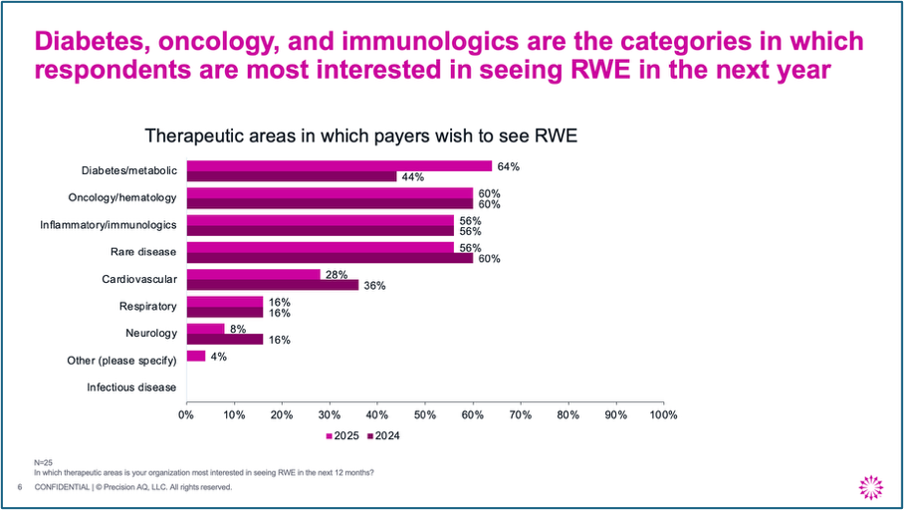
Abbreviation: RWE, real-world evidence.
These 4 areas dominate not simply because they include expensive therapies but because each one presents a distinct set of access questions that remain unresolved by registrational trials:
- Diabetes and metabolic disease: Plans need to understand real-world utilization patterns, adherence, and economic impact across rapidly expanding patient populations.
- Oncology: Payer decisions routinely involve small populations, high-cost regimens, and evolving standards of care where trial evidence leaves practical gaps that are difficult to close quickly.
- Rare disease: RWE often functions less as traditional payer-support evidence and more as market-shaping evidence, helping to identify patients earlier, characterize the diagnostic journey, estimate burden of illness, and define unmet need before a product’s access narrative is fully formed.
- Immune/inflammatory conditions: Questions center on persistence, sequencing, adherence, and long-term cost management.
The common thread is that payers face uncertainty about which patients will receive therapy, how long they will remain on treatment, whether outcomes in trial populations translate to managed care populations, and how the intervention changes total cost of care. For manufacturers, the practical implication is that RWE should be treated as a strategic access asset, customized to the specific questions a given disease state presents, rather than as a generic evidence generation exercise applied uniformly across the portfolio.
Timing of Real-World Evidence
Be Prepared to Share Evidence Early
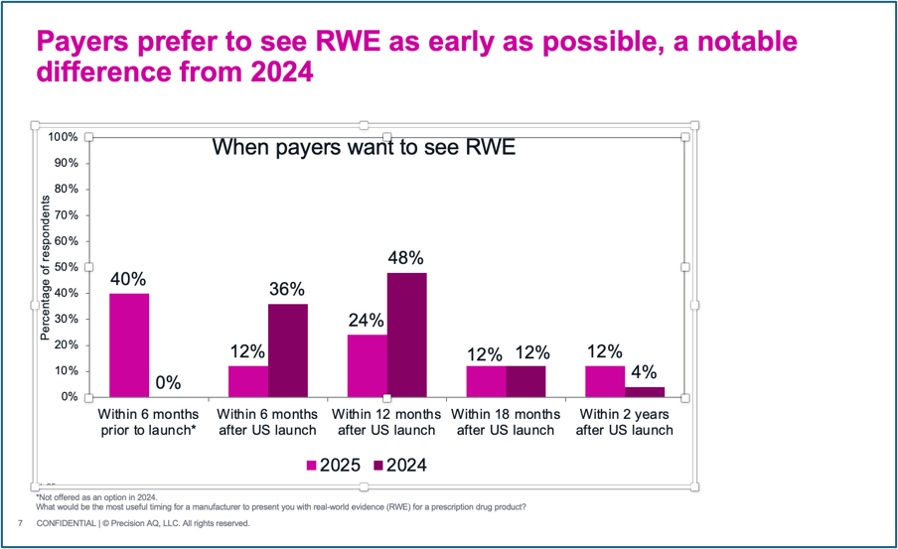
Payer expectations for RWE timing are earlier than many manufacturers may have previously anticipated (Figure 2). Forty percent of respondents said the most useful point for a manufacturer to present RWE is within 6 months of launch, which likely reflects interest in disease burden studies. An additional 24% preferred within 12 months of US launch, whereas 12% selected within 6 months of launch. The remaining respondents were split between 18 months and 2 years after launch (at 12% each). Separately, 92% of respondents said their organizations reevaluate coverage policy on an annual cycle, and 84% reported reviewing formulary placement annually, with the remainder reviewing as-needed or when new products enter the market.
Payers want evidence early, but the most meaningful postlaunch RWE—particularly comparative real-world safety and effectiveness—often requires 2 to 3 years of accumulation before it becomes robust. To provide evidence that meets payer timelines, manufacturers need an RWE roadmap in place before launch, with early-phase evidence focused on disease burden, natural history, patient identification, treatment patterns, and population sizing, followed by more mature postlaunch work on adherence, safety, effectiveness, resource utilization, and cost. The first 6 to 12 months after launch should be treated as a period for establishing credibility by demonstrating to payers that the evidence plan is aligned to their decision-making windows. If evidence becomes available only after a plan's annual review cycle has closed, its practical value may diminish even when the study itself is methodologically sound. Early RWE planning should also manage payer expectations, helping them understand what type of evidence is realistically available at each stage of the product life cycle, rather than overpromising what cannot yet be generated.
The Types of RWE Studies Payers Want to See
Match the Study Design to the Payer Question
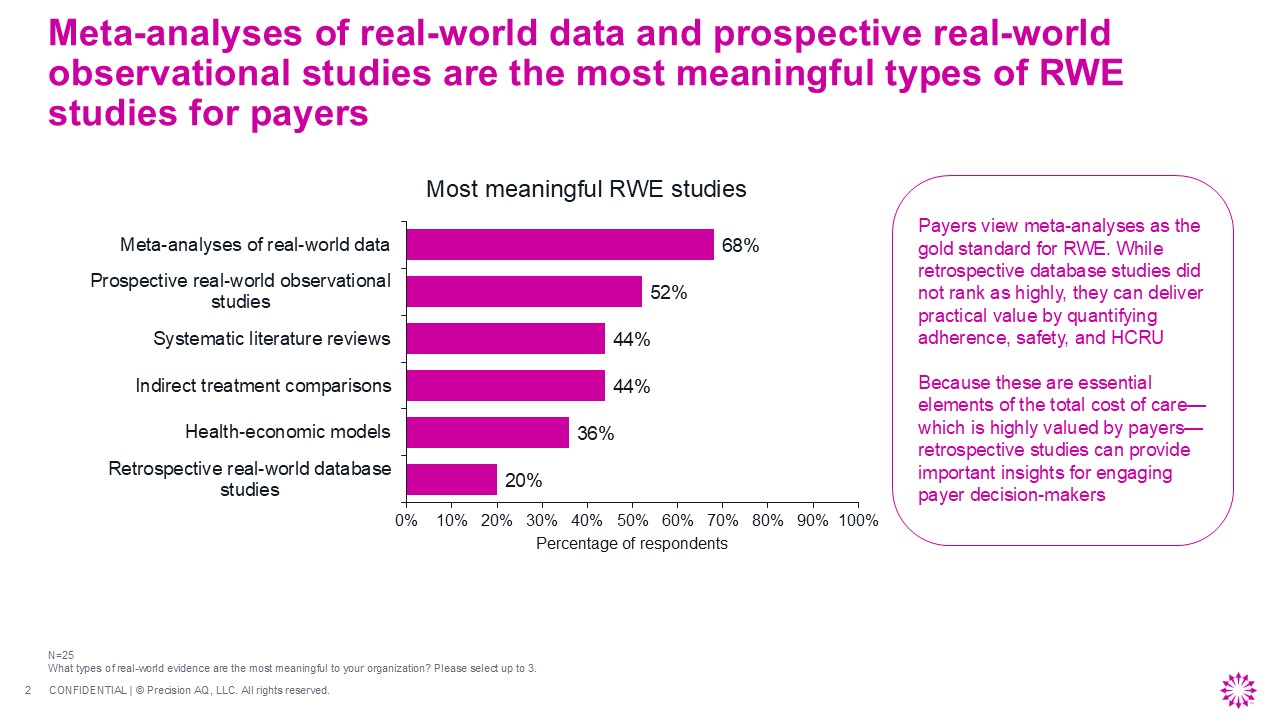
When asked which types of RWE are most meaningful, 68% of payers selected meta-analyses of real-world data (Figure 3). Prospective, real-world observational studies followed at 52%. Systematic literature reviews and indirect treatment comparisons each drew 44%, health-economic models registered at 36%, and retrospective real-world database studies ranked lowest at 20%. These results suggest that payers place a premium on evidence that either synthesizes across multiple datasets or generates prospective observational insight under real-world conditions.
The lower ranking of retrospective database studies should not be read as a dismissal; these studies remain strategically important when tied to the right end point and payer question, and continue to support health-economic modeling and evidence synthesis, including in meta-analyses and systematic literature reviews. Claims-based retrospective work can also quantify adherence, persistence, resource utilization, cost, and treatment patterns, all of which feed into total cost of care, a concept that carries weight with payer decision-makers. The more instructive takeaway is that the “best” study type depends on the business question, not on a fixed ranking of methods. Claims data may be well suited for adherence, utilization, and cost analyses; electronic medical records, registry, chart review, lab data, or prospective observational designs may be necessary when the relevant end point demands clinical detail, disease severity, diagnostic journey, or subpopulation granularity. Manufacturers should begin with the payer question, assess whether the available data source can credibly answer it, and then select the design accordingly. Feasibility analysis, conducted before committing to a study, is a key element of the evidence generation plan: confirming that the data source contains enough patients, the right end points, adequate follow-up, and sufficient clinical detail to support the intended analysis. Meta-analyses and evidence synthesis remain valuable, but they are most useful when they help organize existing evidence around a specific payer decision rather than simply aggregate heterogeneous findings.
The Threshold for Meaningful RWE
Design RWE to Demonstrate Both Clinical Differentiation and Plan-Level Financial Consequence, Not One Alone
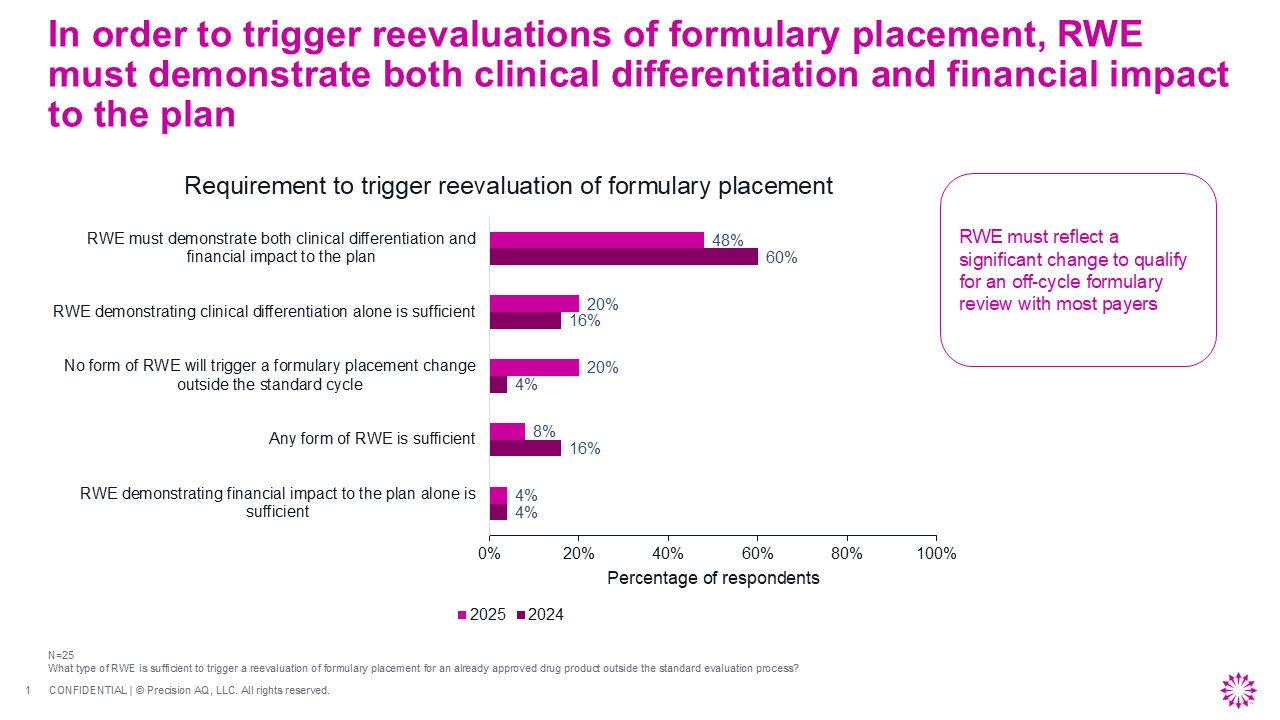
When asked what type of RWE could trigger a reevaluation of formulary placement for an already approved product outside the standard evaluation process, 48% of respondents said RWE must demonstrate both clinical differentiation and financial impact to the plan (Figure 4). Twenty percent said clinical differentiation alone would suffice, 4% said financial impact alone, and 20% said no form of RWE would trigger an off-cycle review. Only 8% said that any form of RWE would be sufficient to trigger a review. The bar for off-cycle reconsideration is demanding, with most payers requiring a clinical difference paired with economic relevance before they will act outside their normal review cadence.
The implication for evidence planning is that “economic value” should not be framed narrowly as drug cost offset. Payers appear to evaluate whether a product changes outcomes, utilization, and total cost of care in the populations they actually manage. While high-cost utilization outcomes, such as hospitalizations and emergency department visits, resonate with payers, these end points lose credibility if they are not presented alongside pharmacy costs and overall impact on total cost of care. Isolated utilization reductions, particularly low-cost events like office visits, are often viewed with skepticism when divorced from a broader economic context. Payers find total cost of care more compelling than single end points, favoring evidence that demonstrates how a product influences resource use, downstream costs, avoidable events, and population-level management. Among utilization measures, hospitalization reduction stands out as especially relevant because it unites clinical benefit and economic consequence within a single, meaningful outcome. Clinical differentiation alone may not be enough if payers cannot connect it to a managed care decision; manufacturers need to show not only that outcomes improve, but why those improvements matter for coverage, formulary placement, or utilization management. The most persuasive RWE packages anticipate payers’ skepticism, transparently addressing limitations, bias, data completeness, patient selection, comparator choice, end point validity, and generalizability before the payer asks.
The Top Challenges Payers Face in Using RWE
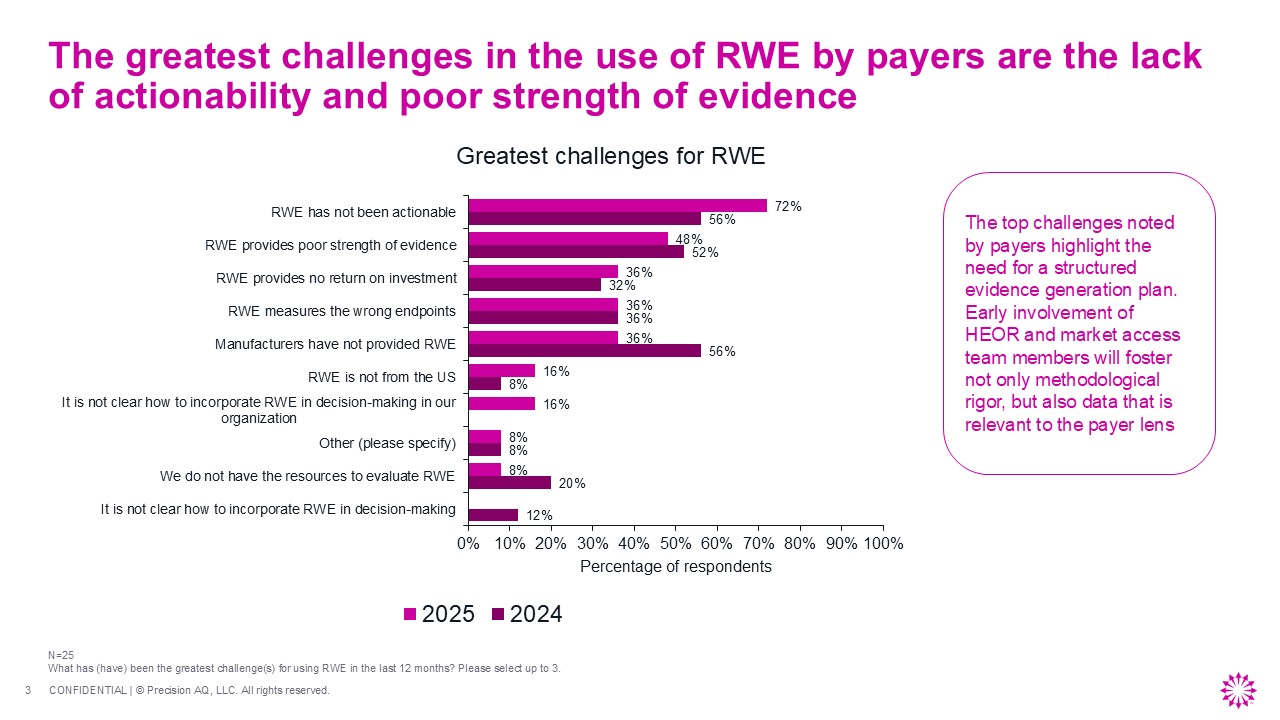
RWE Must Be Actionable, Comparative, and Relevant to the Payer's Own Population and Decision Needs
Lack of actionability was identified as the top challenge by payers (Figure 5). Seventy-two percent of respondents selected this as the greatest RWE challenge in the last 12 months. Poor strength of evidence followed at 48%. Wrong end points, no return on investment, and the absence of manufacturer-provided RWE each stood at 36%. The concentration of responses around actionability and evidence quality indicates that the barrier is not a lack of payer interest in RWE, but a persistent gap between what manufacturers present and what payers can apply to a decision.
These results suggest that failures of RWE in practice center on trust and translation. Payers do not generally dismiss RWE as a category, but question whether manufacturer-funded studies are biased, whether the selected population is relevant to their membership, whether the end point matters, or whether the methods are transparent. RWE presented without end points that map to operational decisions, such as hospitalization or total cost of care, will be discounted regardless of its methodological quality. Evidence that relies on non-US data, uses promotional language, or fails to distinguish product-specific value from a class effect will face similar skepticism. Generalizability remains a persistent interpretation problem: Payers must understand whether the study population resembles their covered lives and whether the data source is appropriate to the question being asked. Single-study evidence is inherently less persuasive than consistent findings replicated across multiple datasets, populations, and care settings.
Manufacturers may also overestimate how much time payers can spend interpreting complex studies; concise communication, clear summaries, and transparent statements of relevance are not optional. A structured approach is needed to clearly communicate evidence that explains data source selection, patient identification, comparator rationale, end point relevance, limitations, and applicability in a format that allows a payer to assess quickly whether the evidence warrants deeper review.
What Makes RWE Effective or Ineffective
Present Peer-Reviewed, US-Sourced, and Comparative Evidence With Clear Economic Meaning and Transparent Methods
In a free response question, payers shared that effective RWE communications were characterized by scientific rigor, published and peer-reviewed sources, clear inclusion and exclusion criteria, and evidence that extends meaningfully from the labeled indication into outcomes. On the other hand, manufacturer engagement falls flat when evidence comes only from outside the US, or measures end points that are not relevant to the payer’s decision framework. And some manufacturers have failed to provide RWE at all.
Effective RWE
“Product demonstrates RWE that extends from its labeled indication. For example, RWE that demonstrates reduced health care resource utilization due to fewer cardiovascular events based on a label that says that drug is used for resistant hypertension.” - Pharmacy director, PBM
“Scientific rigor and relevant information that may change the management of the drug. So, we need RWE from published peer-reviewed studies. A great example was a manufacturer who provided a published RWE study that showed that the treatment was cost effective. Based on that, we changed the status of that drug from nonpreferred to preferred status.” - Medical director, regional plan
Ineffective RWE
“Similar to placebo-controlled trials, RWE in a vacuum in usually not helpful. It has to be comparative and actionable and fill a clear unmet need using the correct end points (eg, hospitalization, emergency room).” - Pharmacy director, PBM
“Sometimes lack of peer review or promotional bias makes it ineffective.” - Pharmacy director, national plan
The deeper principle is that the most credible RWE story is cumulative, transparent, and reproducible. Payers are more persuaded when manufacturers can demonstrate similar results across multiple datasets, patient populations, demographics, and care settings. This matters especially because payers may distrust a single manufacturer-sponsored analysis or discount evidence that does not resemble their own covered population. Evidence becomes more credible when manufacturers acknowledge limitations openly, explain generalizability, and, when possible, incorporate payer-relevant or payer-owned data into the analysis. The practical recommendation is straightforward: Manufacturers who treat RWE communication as a transparency exercise, showing the payer exactly how the study was designed, why the data source was chosen, what the limitations were, and how the results apply to managed care populations, will consistently outperform those who treat it as a promotional deliverable. Economic outcomes, particularly cost-effectiveness and total cost of care, remain the most underrepresented and most requested categories of evidence. Manufacturers who can fill that gap with credible, published, US-sourced data will hold an advantage in coverage conversations.
Treat RWE as a Planned Access Asset, Not a Late-stage Supporting Exhibit
Practical Steps for Pharmaceutical Manufacturers
Payers are receptive to RWE but will not reward it for simply existing. The most powerful evidence that shapes decision making must be timely, credible, comparative, economically relevant, and framed around the decisions a payer needs to make. The following recommendations reflect both the survey data and the practical realities of how payers evaluate and apply RWE.
Build the evidence plan before launch. Sequence RWE generation to match payer review cycles and to support the first coverage and formulary discussions, not merely later life cycle communications. Early-phase evidence should address disease burden, patient identification, natural history, and population sizing; postlaunch work should target adherence, safety, effectiveness, resource utilization, and cost. The most meaningful comparative evidence may take 2 to 3 years to mature, which makes early planning essential rather than optional.
Anchor every study to a payer decision, not to general scientific interest. Prioritize end points and designs that demonstrate comparative clinical relevance and plan-level economic consequence, especially in therapeutic areas where payer demand is highest. Begin with the payer question, confirm that the available data can answer it, and then select the study design. RWE that cannot be connected to a specific coverage, formulary, or utilization management decision is unlikely to influence action.
Raise the communication standard. Use peer-reviewed, methodologically clear, nonpromotional materials that explain why findings are applicable to US managed care populations, how the comparator was handled, and why the outcomes should matter to a formulary or coverage review. Anticipate payer skepticism by addressing limitations, bias, patient selection, data source fit, and generalizability before the payer raises them. When possible, demonstrate consistency of findings across multiple datasets and care settings.
Integrate RWE into the access strategy from the start. RWE is most likely to influence decisions when health economics, medical affairs, market access, and commercialization teams shape the questions, end points, timing, and communication plan together. The evidence plan should not be a standalone health economics and outcomes research workstream; it should be a coordinated element of the product's access strategy, with clear ownership, defined milestones, and explicit alignment to payer decision calendars and information needs.
References
- US Food and Drug Administration. Real-world evidence. June 3, 2026. Accessed May 13, 2026. https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence
- US Food and Drug Administration. FDA use of real-world evidence in regulatory decision making. June 3, 2026. Accessed May 13, 2026. https://www.fda.gov/science-research/real-world-evidence/fda-use-real-world-evidence-regulatory-decision-making
- US Food and Drug Administration. FDA eliminates major barrier to using real-world evidence in drug and device application reviews. December 15, 2025. Accessed May 13, 2026. https://www.fda.gov/news-events/press-announcements/fda-eliminates-major-barrier-using-real-world-evidence-drug-and-device-application-reviews
- Lockhart CM, Powers E, Sweet B, Gleason PP, Brixner D. AMCP real-world evidence standards: overcoming barriers to using real-world evidence in US payer decision-making. J Manag Care Spec Pharm. 2025;31(12):1230-1236. doi:10.18553/jmcp.2025.25108



