Advanced Heart Failure Trends in the Cath Lab: Hemodynamics, MCS, and Biopsy Workflows
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Mark R. Hofmeyer, MD, MS, FACC, is Program Director of the Advanced Heart Failure and Transplant Cardiology Fellowship Program at MedStar Washington Hospital Center, Medical Director of the Advanced Heart Failure IMC, and Associate Professor of Medicine at the Georgetown University School of Medicine. He disclosed no relevant financial relationships.
Dr. Hofmeyer can be contacted at mark.hofmeyer@medstar.net.
 At CRT 2026 in Washington, DC, advanced heart failure specialist Mark R. Hofmeyer, MD, MS, FACC, presented “Current Trends in Advanced Heart Failure: How Does It Impact the Cath Lab, MCP, Right Heart Cath, and Biopsies?” during the March 8th Nurses and Technologists session.
At CRT 2026 in Washington, DC, advanced heart failure specialist Mark R. Hofmeyer, MD, MS, FACC, presented “Current Trends in Advanced Heart Failure: How Does It Impact the Cath Lab, MCP, Right Heart Cath, and Biopsies?” during the March 8th Nurses and Technologists session.
Dr. Hofmeyer framed advanced heart failure (HF) as a moving target with overlapping but non-identical definitions across major societies, yet a shared clinical reality: severe symptoms despite optimal medical therapy that often drive recurrent hospitalizations and marked functional decline. He centered his remarks on Stage C and Stage D HF, where cath lab-enabled interventions and systems of care can most directly change patient trajectories.
A key theme was the limits of symptom-based assessment and the cath lab’s growing role in providing objective hemodynamic clarity. Dr. Hofmeyer emphasized that congestion and hemodynamic compromise are frequently underappreciated until late. “Patients can appear more well than they truly are,” he said. “Relying on the traditional physical exam and on patients’ symptom narratives doesn’t always tell the full story. We still get burned if we don’t have objective, hemodynamic data.” This framing matters operationally for cath lab teams because it shifts the clinical “north star” from what the patient reports to what continuous or invasive hemodynamics show, and it sets up the rationale for more device-based monitoring and intervention.
Dr. Hofmeyer described how HF therapy is pivoting from medication-only optimization to catheter-based and device-based strategies that increasingly intersect with interventional workflows. He contrasted the historical pharmacologic “pillars” (beta blockers, angiotensin-converting enzyme inhibitors [ACE] inhibitors, mineralocorticoid receptor antagonists [MRAs]) with the modern landscape that added “one more pillar” over the past decade, then made the broader point that the next wave is procedural: “Pharmacologic therapies are not the future of heart failure treatment. It’s really going to be catheter-based therapies and device-based therapies.”
Hemodynamics as Management Guidance
Dr. Hofmeyer highlighted invasive and implantable hemodynamic monitoring as a foundational trend. Using the CardioMEMS HF System made by Abbott, a pulmonary artery (PA) pressure monitor, as the anchor example, he described the clinical logic familiar to cath lab staff: if PA catheters help guide inpatient management, leaving a sensor can extend hemodynamic insight longitudinally and allow real-time therapy adjustment. He summarized trial-level benefits from the GUIDE-HF trial, noting a 19% reduction in cumulative hazard and a 28% reduction in heart failure hospitalizations, and he urged the audience to think of pressure-guided care as an active therapy: monitoring plus response changes outcomes. He also referenced the Corvella Sensor by Endotronix as another hemodynamic platform showing similar reductions in hospitalizations and all-cause mortality.
A newer investigational approach, the Norm System by FIRE1, shifts from pressure sensing to inferior vena cava (IVC) volume measurement, paralleling how clinicians use IVC ultrasound distensibility/collapsibility to estimate right atrial pressure. He noted good correlation with CT-sized IVC measurements and pointed to future enrollment in the FUTURE-HFII trial. For cath lab teams, the implication is a broader menu of implants and follow-up pathways: more patients with implanted hemodynamic sensors, more troubleshooting/quality assurance around data integrity, and greater need for well-defined escalation protocols that turn numbers into actions.
Structural and Device Therapies Entering the Advanced HF Toolkit
Dr. Hofmeyer surveyed several catheter-based therapies that may alter cath lab case mix and imaging/coordination requirements. He briefly described catheter-based ventricular reconstruction, referencing the AccuCinch system by Ancora Heart, originally designed to address functional mitral regurgitation (MR) but more practically repurposed as a percutaneous left ventricular remodeling system now in trial enrollment.
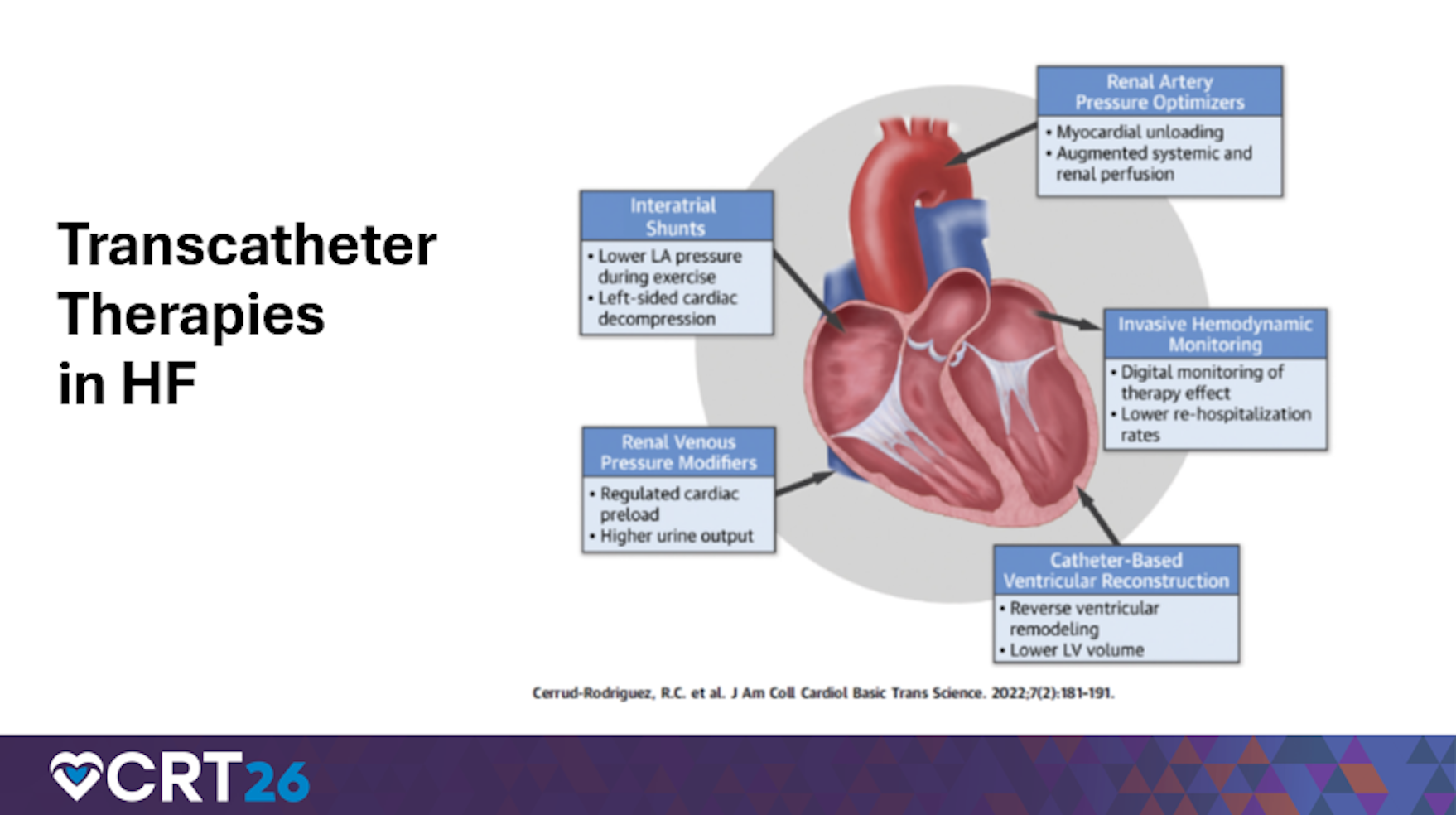
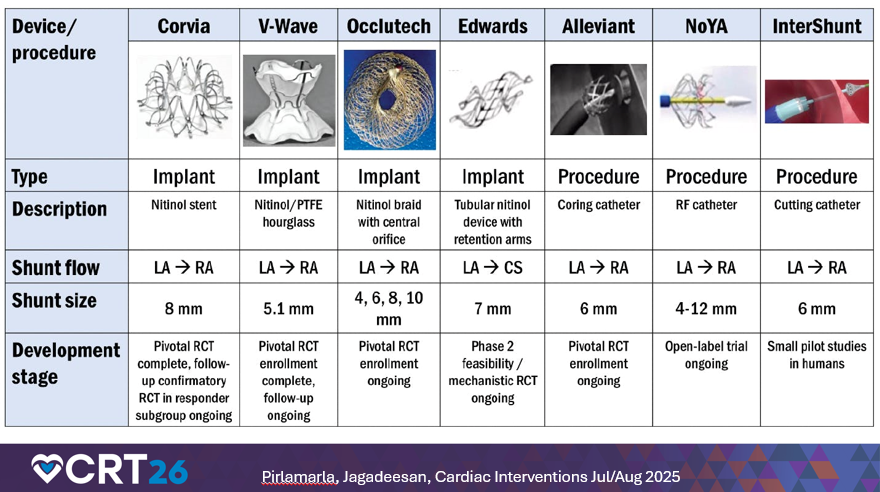
He also discussed intra-atrial shunts for heart failure with preserved ejection fraction (HFpEF) patients with elevated left atrial pressures and exertional symptoms, involving creating a small left-to-right shunt to offload left atrial (LA) pressure and volume. He noted multiple devices in production and study, reinforcing that HFpEF management is increasingly procedural and may require cath lab readiness for structural workflows, device-specific setup, and post-procedure monitoring.
Another key driver of cath lab demand is the rise in cardiac amyloidosis recognition across HFpEF and heart failure with reduced ejection fraction (HFrEF). Dr. Hofmeyer emphasized that diagnosis often requires myocardial biopsy to demonstrate amyloid deposition, directly linking advanced HF trends to increased volumes of right heart cath with endomyocardial biopsy and associated operational needs: coordination, specimen handling, and complication preparedness.
Shock Teams, Mechanical Circulatory Support, and What “Advanced HF” Means in the Lab
Transitioning from Stage C to Stage D HF, Dr. Hofmeyer underscored the expanding role of shock teams and protocolized escalation in improving outcomes. He noted that shock teams have been associated with better 30-day survival for both acute myocardial infarction (MI) shock and decompensated chronic HF shock, alongside increased use of PA catheters and advanced mechanical circulatory support (MCS).
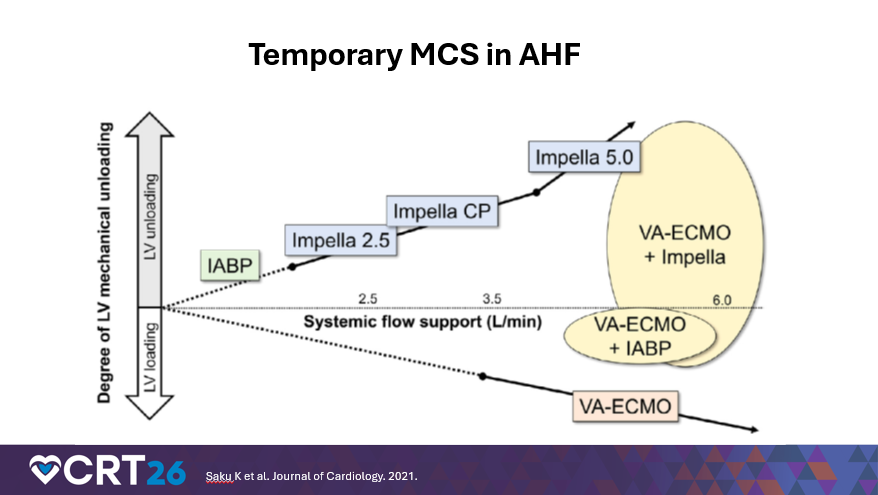
For interventionalists, nurses, and technologists, his operational message was direct: temporary MCS is no longer confined to high-risk PCI. Devices such as an intra-aortic balloon pump (IABP), Impella (Abiomed), and surgically placed Impella 5.5 are increasingly used to stabilize and bridge advanced HF patients to durable therapy (LVAD or transplant). He also delivered a practical hemodynamic caution with immediate implications for lab/ICU co-management: “If you put a patient on VA ECMO [venoarterial extracorporeal membrane oxygenation], it actually increases afterload,” Dr. Hofmeyer said. “So we always want to have some type of LV [left ventricular] unloading device in combination with VA ECMO.”
He added a systems-level driver: changes to the 2018 allocation system have increased utilization of temporary support, because IABP or percutaneous temporary left ventricular assist device (LVAD) can upgrade transplant status (to Status 2, as he noted), accelerating demand for device placement and management pathways.
Downstream Impact: More Biopsies, More LVAD Cath Lab Work
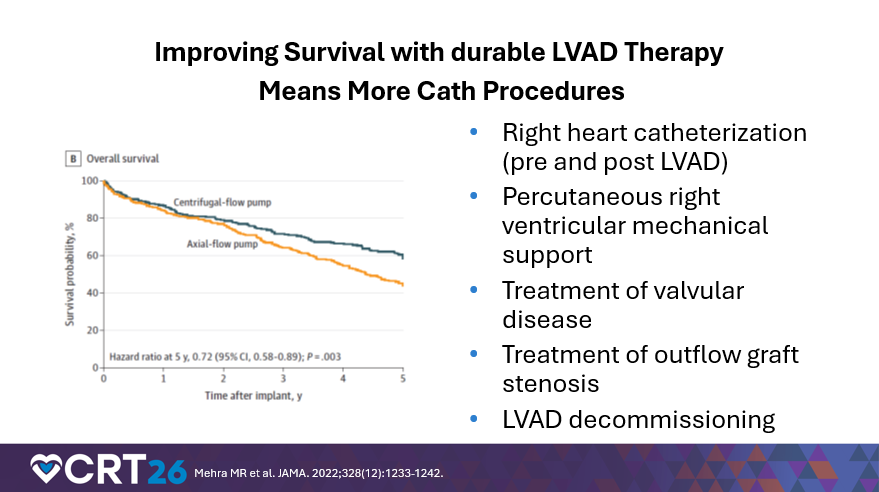
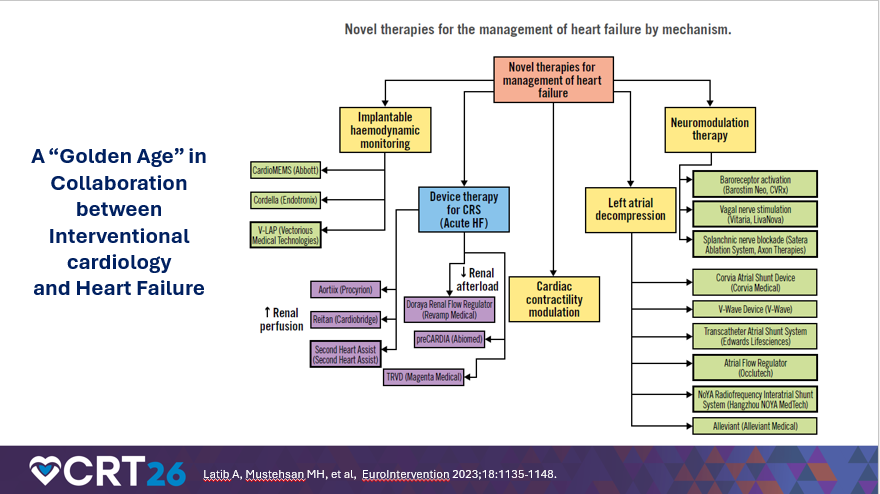
Finally, Dr. Hofmeyer described how growth in cardiac transplantation and improved durability of long-term LVAD therapy translate into more cath lab encounters over time. With more transplants comes greater need for biopsy surveillance. With better LVAD outcomes—he referenced five-year survival improvements from the MOMENTUM trials experience and post-study survival in the 70-80 percent range at five years—comes a larger population living longer with devices, driving more right heart catheterizations, more management of valvular disease (including aortic insufficiency), evaluation/treatment of outflow graft stenosis, and occasional LVAD decommissioning in the subset with LV recovery. Dr. Hofmeyer closed by emphasizing collaboration: a “golden age” of teamwork between advanced HF and interventional services, as catheter-based therapies become central to contemporary HF care.
Cath lab takeaways for nurses, technologists, and interventionalists:
- Expect continued growth in hemodynamic monitoring implants and workflows that require rapid, protocolized responses to abnormal data.
- Build and rehearse shock-team pathways and MCS escalation, including LV unloading strategies with VA ECMO.
- Plan for increasing volumes of right heart catheterization + biopsy (amyloid and post-transplant) and long-term LVAD-related cath lab work (hemodynamics, valve disease, graft issues).