


Advancing Coronary Intervention With Terumo’s Takeru™ PTCA Balloon Dilatation Catheters
A Clinical Experience Across Complex Lesions and Intravascular Lithotripsy
A Clinical Experience Across Complex Lesions and Intravascular Lithotripsy
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Ghulam Mujtaba Ghumman, MD1; Zaid Al-Jebaje, MD2
1Cardiovascular Disease Fellow, Mercy Health Saint Vincent Medical Center, Toledo, Ohio;
2Interventional Cardiologist, Mercy Health Saint Vincent Medical Center, Toledo, Ohio

Background
As the complexity of coronary artery disease in patients undergoing percutaneous coronary intervention (PCI) continues to increase, the need for advanced tools in lesion preparation and post-stent optimization becomes ever more critical. Complex coronary lesions, severe calcifications, bifurcation disease, and in-stent restenosis remain technically challenging scenarios, often necessitating a combination of precision, power, and deliverability in the devices used. The Takeru™ PTCA Balloon Dilatation Catheter by Terumo Interventional Systems represents a significant innovation in this field. Built with a low entry and crossing profile, the Takeru™ catheter is engineered for optimized lesion access, particularly in complex or previously stented vessels.1 The system offers best-in-class pushability and trackability, crucial for navigating tortuous and calcified coronary anatomies.1 Importantly, the tight re-wrap mechanism allows for superior re-crossability and lesion engagement, especially in multistep interventions.1
Takeru™ balloons are available in both semi-compliant (SC) and non-compliant (NC) variants, enabling tailored use throughout the PCI process — from gentle pre-dilatation in delicate branches to high-pressure post-dilatation in rigid calcific beds. In combination with adjunctive technologies such as intravascular lithotripsy (IVL), the Takeru™ system offers exceptional support for complete lesion preparation and optimal stent expansion. This article highlights three real-world complex PCI cases in which Takeru™ balloon catheters were utilized, including their role in IVL-supported lesion preparation, complex coronary lesion crossing, and bifurcation stenting strategies. These cases illustrate the clinical utility and design advantages of the Takeru™ system in overcoming procedural hurdles and achieving favorable angiographic and patient outcomes.
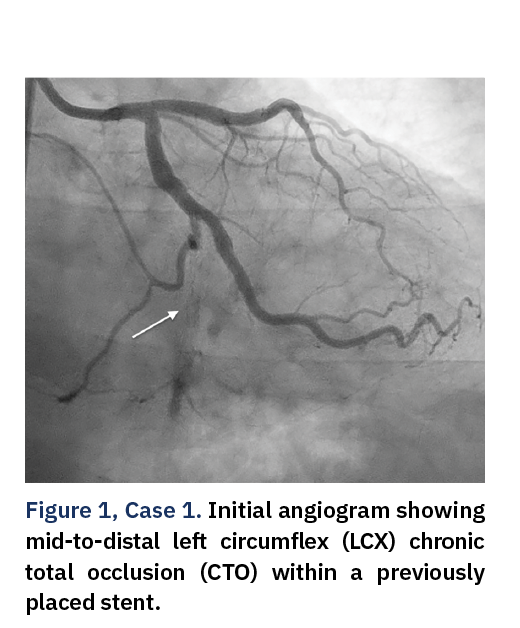
Case 1: CTO of the LCX to LPDA With In-Stent Restenosis in an Old Stent
A 57-year-old male with chronic stable angina and a history of smoking presented with a chronic total occlusion (CTO) of the mid-to-distal left circumflex artery (LCX) extending to the left posterior descending artery (LPDA), involving a previously implanted stent (Figure 1).
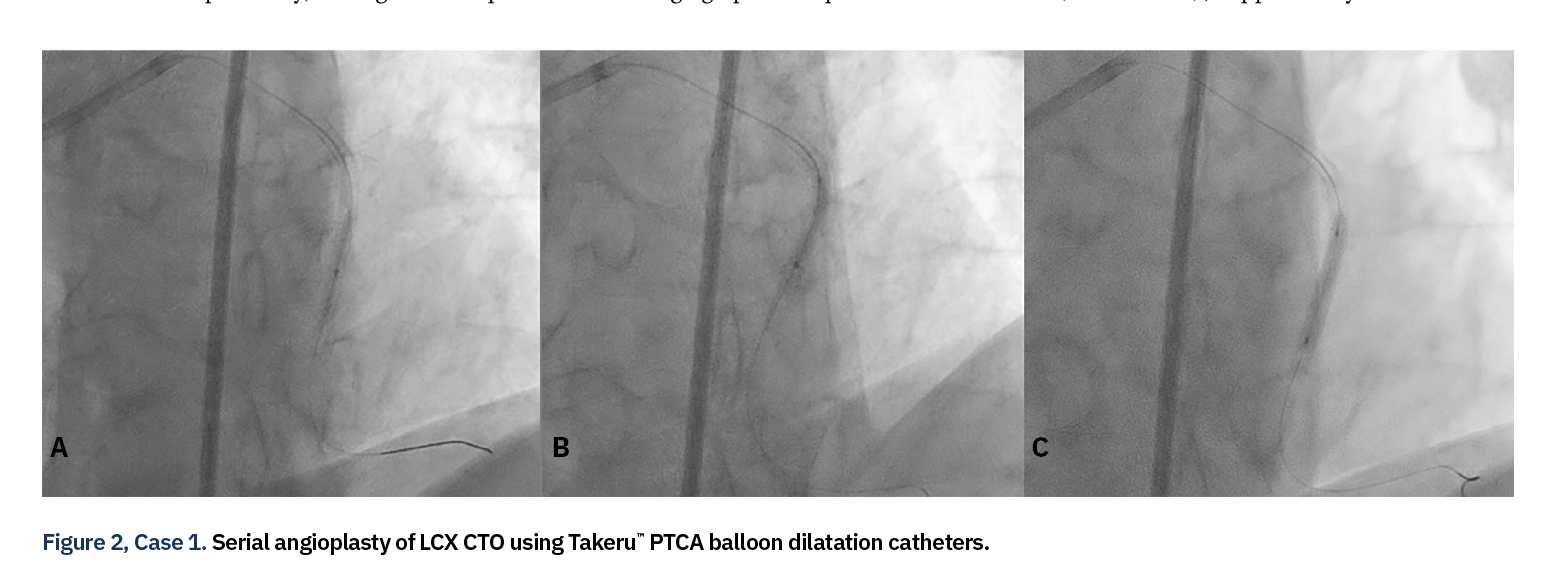
Right femoral access was obtained with placement of an 8 French (Fr), 35 cm sheath, and the left coronary system was engaged using an Extra Back-Up (EBU) 4.0 guide catheter. An initial attempt to cross the CTO with a Minamo™ guidewire (Asahi Intecc) was unsuccessful; however, successful lesion crossing was eventually achieved using a Gaia™ guidewire (Asahi Intecc), supported by a Corsair® Pro XS microcatheter (Asahi Intecc). Sequential balloon dilatation was then performed using a series of Takeru™ semi-compliant (SC) balloons. A 1.5 mm x 20 mm SC Takeru™ balloon was inflated once to 20 atmospheres (atm), followed by a 2.0 mm x 20 mm SC Takeru™ balloon with two inflations to 14 atm. A 2.5 mm x 20 mm SC Takeru™ balloon was then inflated once to 14 atm (Figure 2).
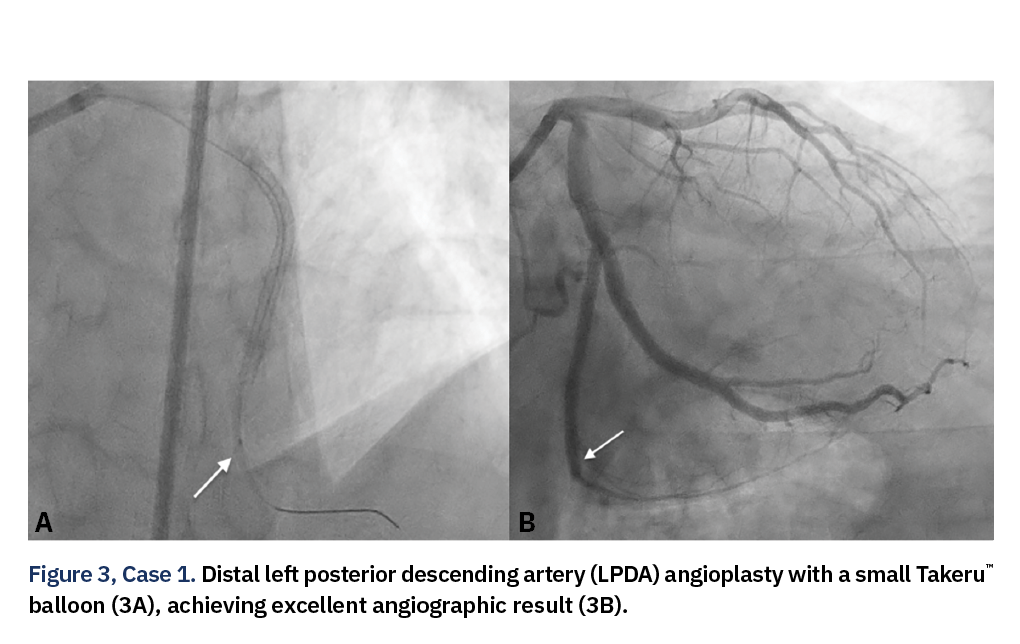
Then we were able to advance intravascular ultrasound (IVUS), which confirmed in-stent restenosis as the CTO mechanism. Further lesion preparation was carried out using a 3.0 mm x 21 mm non-compliant (NC) Takeru™ balloon with two inflations to 12 atm. A 2.5 mm x 48 mm Resolute™ Onyx™ drug-eluting stent (Medtronic) was deployed and proximally post-dilated using the same 3.0 mm Takeru™ NC balloon at 14 atm. A final small balloon angioplasty of the LPDA was performed just distal to the stent edge using the 1.5 mm Takeru™ SC balloon (Figure 3A). This was followed by a distal intracoronary nitroglycerin injection via microcatheter to optimize flow, with excellent results (Figure 3B). Hemostasis was achieved at the femoral access site using the Perclose™ closure device (Abbott). The patient tolerated the procedure well, and no complications occurred.
Case 2: Complex Bifurcation PCI in a Morbidly Obese Patient Unfit for CABG
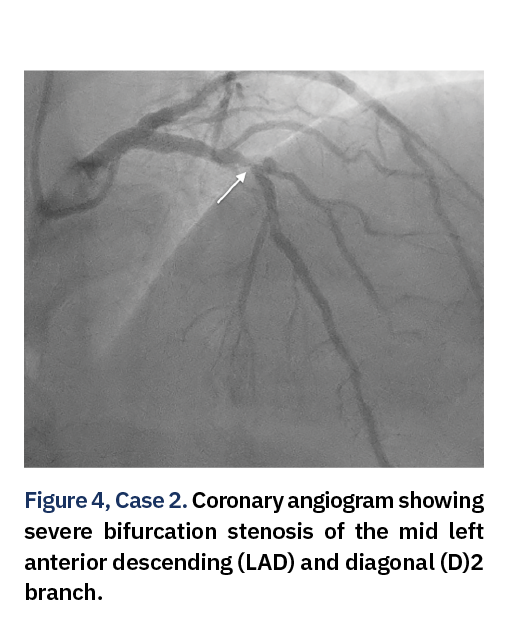
A 70-year-old male with significant comorbidities, including morbid obesity (BMI 61 kg/m2), diabetes, obstructive sleep apnea, and paroxysmal atrial flutter, presented with exertional chest pain and shortness of breath. Stress testing revealed a reversible perfusion defect in the anteroseptal and inferior myocardial territories. Coronary angiography demonstrated a 90% stenosis of the mid left anterior descending (LAD) artery at its diagonal branch (D2) bifurcation, 90% D2 ostial stenosis, and 80% distal LAD stenosis, along with 70% proximal and 80% mid-stenosis in the left circumflex artery (LCX) (Figure 4).
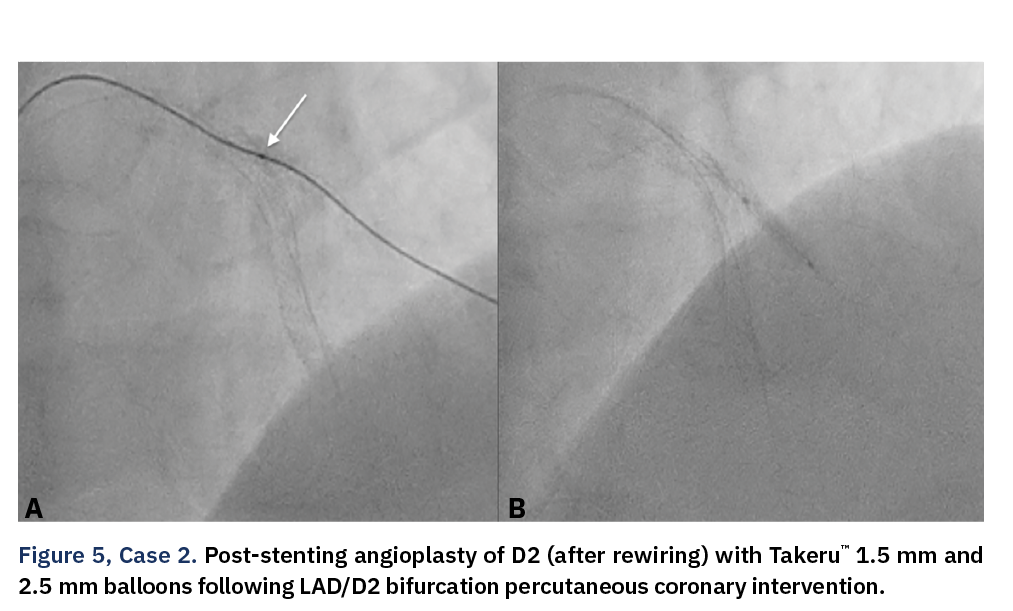
Due to his comorbid state and prohibitive surgical risk, the patient was deemed unsuitable for coronary artery bypass grafting (CABG) and opted for percutaneous revascularization. PCI was initiated via right radial access with a 7 Fr sheath. The coronary engagement was achieved with a 7 Fr EBU 4.0 guide catheter. Both the LAD and D2 were wired, and IVUS was performed for lesion assessment. The D2 lesion was prepped with a 2.5 mm x 20 mm SC balloon (Medtronic). Given the presence of severe calcification in the mid LAD, IVL was performed using a 4.0 mm x 12 mm Shockwave balloon, delivering 6 cycles (60 pulses) at 6 atm. A 2.5 mm x 26 mm drug-eluting stent (Resolute Onyx) was then deployed in the D2, while a 4.0 mm x 21 mm Takeru™ NC balloon was simultaneously placed in the LAD (which was inflated to 12 atm after D2 wire removal). A 4.0 mm x 48 mm drug-eluting stent was then deployed from the proximal to mid LAD and post-dilated proximally with a 5.0 mm x 12 mm NC balloon (Medtronic). After rewiring into the D2 branch, serial balloon angioplasties were performed using a Takeru™ 1.5 mm x 15 mm rapid-exchange (RX) balloon with three inflations to 14 atm, followed by a 2.5 mm x 15 mm Takeru™ NC balloon with a single inflation (Figure 5).
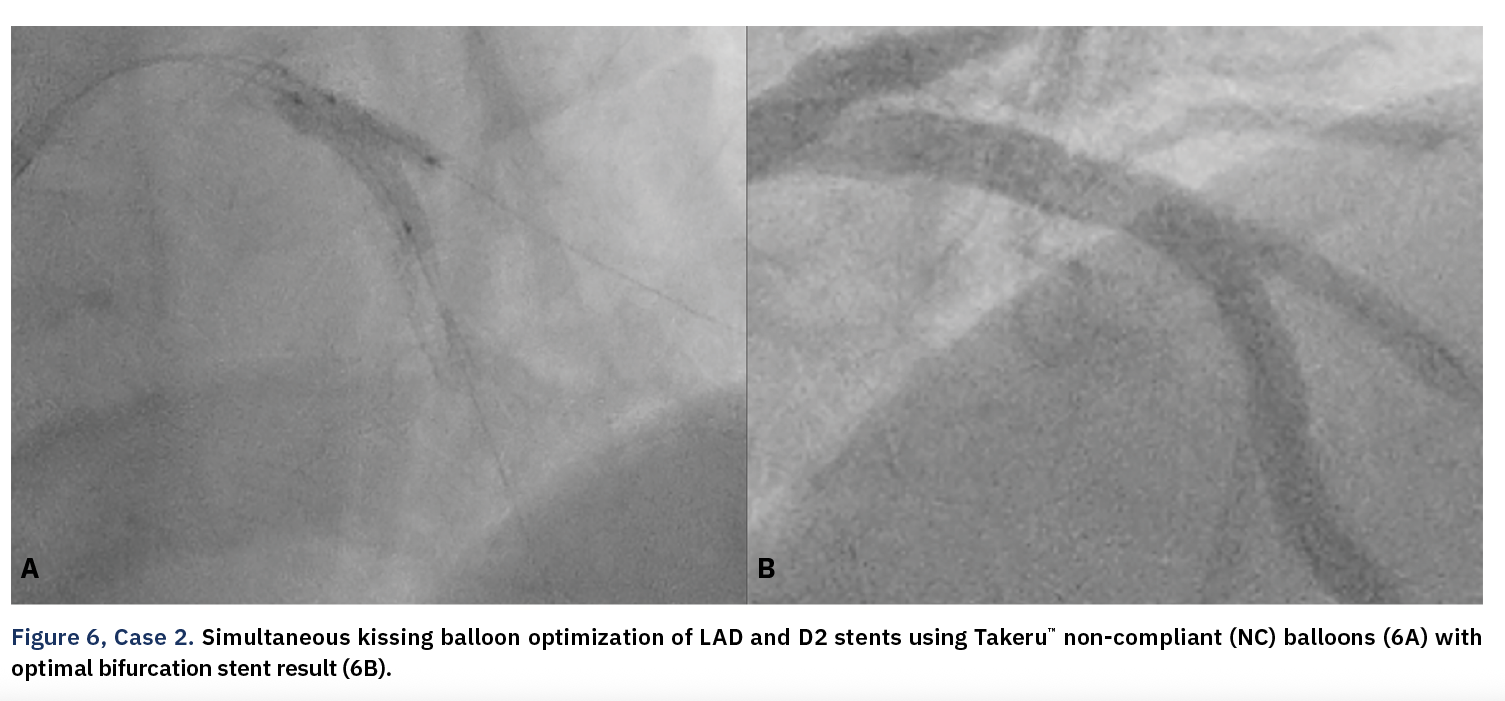
This was followed by a simultaneous kissing balloon optimization of the D2 and LAD stents with Takeru™’s 2.5 mm x 15 mm and 4 mm x 21 mm NC balloons, respectively, with excellent results (Figure 6). The patient tolerated the procedure well without any complications. The patient was discharged home in stable condition with a plan of LCX PCI in the future if symptoms persist.
Case 3: LAD CTO Requiring Lesion Preparation With Takeru™ and Adjunctive IVL
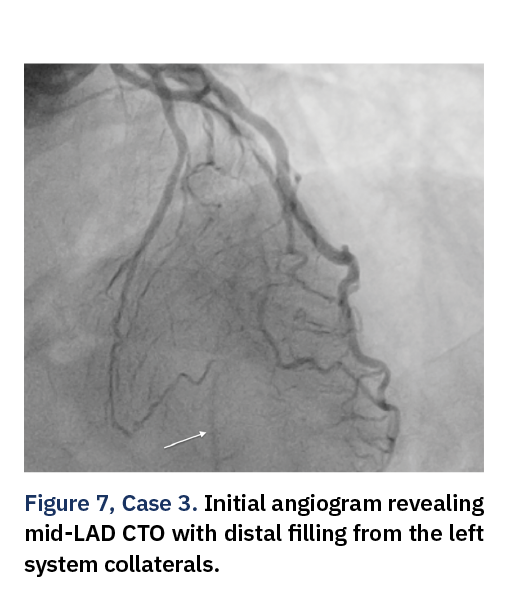
A 54-year-old male with a history of chronic smoking and a known chronic total occlusion of the left anterior descending (LAD) artery presented with recurrent angina. Stress testing revealed a reversible perfusion defect in the anterior and apical segments. The patient was scheduled for elective CTO PCI. Right femoral access was obtained, and an 8 Fr sheath was inserted. The left coronary artery was engaged with an EBU 4.0 guide catheter with an initial angiogram showing a CTO of the proximal LAD with distal filling from left-to-left collaterals (Figure 7).
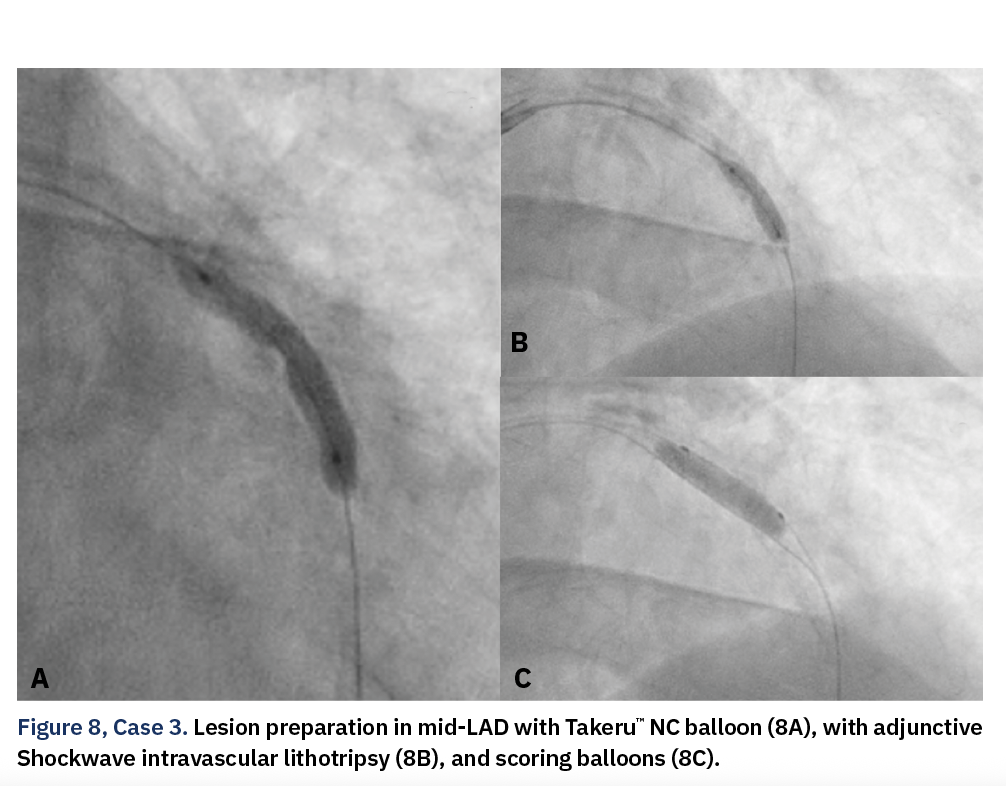
The LAD CTO was crossed with a Fielder® XT wire (Asahi Intecc) supported by a Turnpike® microcatheter (Teleflex). Initial lesion preparation began with sequential balloon angioplasty using 2.0 mm x 20 mm and 2.0 mm x 30 mm SC balloons (Medtronic). IVUS confirmed a severely calcified artery requiring further lesion modification. A 3.5 mm x 21 mm Takeru™ NC balloon was then inflated to 12 atm, followed by IVL with a 3.5 mm x 12 mm Shockwave balloon, delivering 2 cycles (12 pulses) at 6 atm. Additional lesion modification was performed using a 4.0 mm x 15 mm Scoreflex NC balloon (Abbott), inflated to 12 atm (Figure 8).
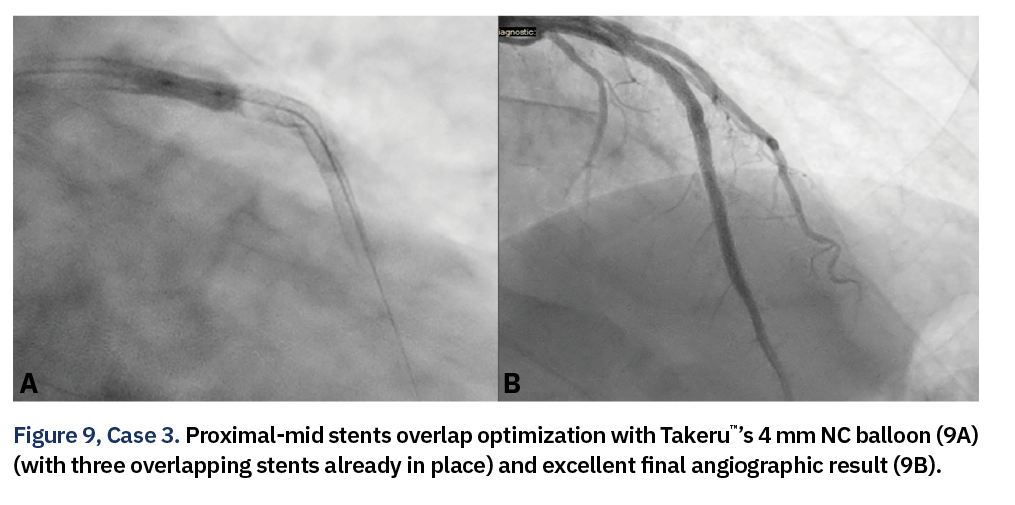
Distal LAD preparation was completed with a 2.75 mm x 21 mm Takeru™ NC balloon (4 inflations to 12 atm) and a 2.75 mm x 21 mm Scoreflex balloon with a single inflation. Stent deployment included a 2.75 mm x 38 mm drug-eluting stent in the distal LAD, a 3.5 mm x 38 mm drug-eluting stent in the mid LAD, and a 4.0 mm x 22 mm drug-eluting stent in the proximal LAD. The mid LAD stent was post-dilated using a 4.0 mm x 21 mm Takeru™ NC balloon at 8 atm, and final optimization at the proximal-mid stent overlap zone was achieved using a 4.0 mm x 8 mm Takeru™ NC balloon, with excellent results (Figure 9). Hemostasis was achieved with a Perclose™ closure device, and the patient experienced no adverse events.
Rationale
These three cases demonstrate the clinical adaptability and engineering strengths of the Takeru™ PTCA balloon catheter system, particularly in the setting of advanced and complex coronary lesions. Across all interventions, the catheter exhibited excellent performance characteristics, beginning with its low crossing profile, which enabled smooth passage through severely stenotic, calcified lesions and in-stent restenotic segments. The system’s superior pushability and trackability, aided by a dual-layer shaft design, allowed the Takeru™ balloon catheter system to navigate tortuous anatomies efficiently, whether accessed through radial or femoral routes. Efficient navigation was especially evident in cases requiring deep intubation or precise support during wire escalation or device delivery. In bifurcation PCI, the tight re-wrap capability proved invaluable by facilitating re-crossability into side branches after main vessel stenting, streamlining procedural workflow and reducing device exchanges. Furthermore, the non-compliant (NC) variants of the Takeru™ balloon consistently delivered high-pressure performance, ensuring effective lesion modification, especially in calcified beds, and optimal stent expansion in both mid- and post-IVL settings. The catheter also integrated seamlessly with adjunctive therapies like IVL and scoring balloons, underscoring the Takeru™’s versatility across a spectrum of lesion types and procedural strategies. Collectively, the Takeru™ system’s technical features translated into improved control, reduced procedural complexity, and enhanced confidence in tackling high-risk interventions, making it a dependable asset in contemporary PCI.
Conclusion
These three cases illustrate the versatility and performance of the Takeru™ PTCA Balloon Dilatation Catheter in complex coronary interventions. From complex coronary lesion crossing and bifurcation stenting to heavily calcified lesions requiring IVL, the Takeru™ system supports effective lesion preparation, precise post dilatation, and successful stent deployment. The availability of both semi-compliant and non-compliant balloon variants further enables clinicians to tailor therapy across the full spectrum of PCI scenarios, ultimately contributing to improved procedural efficiency and patient outcomes.
This case is supported by Terumo Interventional Systems.
Reference
1. TAKERU PTCA Balloon Dilatation Catheter. https://www.terumois.com/products/coronary-intervention-devices/ptca-balloon-dilatation-catheters.html
PM-09785


