


“Pleating Artifact” in Circumflex and Left Main Coronary Arteries Resembling Dissection During PCI
Case report
A 63-year-old male patient presented to our hospital with exercise-induced angina pectoris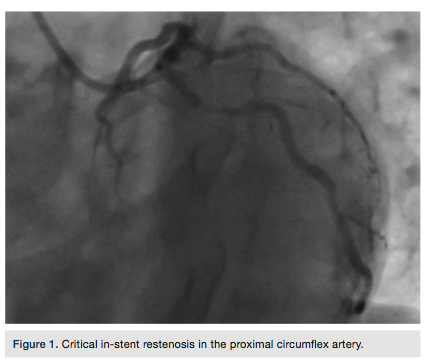 lasting for one month. Four months prior, he had stent placement in the left anterior descending (LAD) and circumflex (Cx) arteries. Coronary angiography showed a critical in-stent restenosis in the proximal Cx artery (Figure 1). Drug-eluting stent implantation through the radial artery was planned to treat the in-stent restenosis of the Cx artery.
lasting for one month. Four months prior, he had stent placement in the left anterior descending (LAD) and circumflex (Cx) arteries. Coronary angiography showed a critical in-stent restenosis in the proximal Cx artery (Figure 1). Drug-eluting stent implantation through the radial artery was planned to treat the in-stent restenosis of the Cx artery.
A Judkins left guiding catheter and soft guide wire were selected for the procedure. The stent (2.75 x 18 mm) could not turn into the Cx artery, due to the acute angle of the Cx origin from the left main coronary artery (LMCA) and inadequate support of the delivery system. An extra back-up (EBU) guiding catheter and an extra-support guide wire were utilized. A prominent filling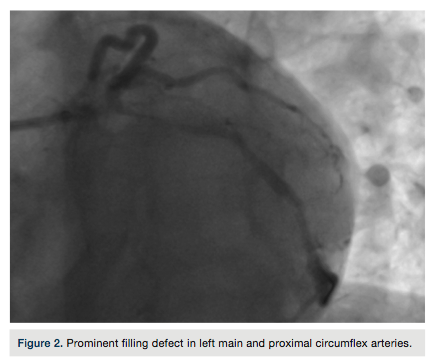 defect in the LMCA and proximal CX artery was encountered that was refractory to nitroglycerin and resembled coronary dissection, due to LMCA trauma from the EBU catheter (Figure 2). The patient had no clinical symptoms or EKG changes. A “pleating artifact” in the LMCA and Cx artery, induced by the stiff structure of the extra support guidewire, was felt to be likely due to the acute angle of the origin of CX artery from the LMCA. The guide wire was partially withdrawn and the filling defect decreased (Figure 3). A stent was appropriately placed into the in-stent restenosis without any complication. The filling defect completely disappeared after complete withdrawal of the guide wire (Figure 4).
defect in the LMCA and proximal CX artery was encountered that was refractory to nitroglycerin and resembled coronary dissection, due to LMCA trauma from the EBU catheter (Figure 2). The patient had no clinical symptoms or EKG changes. A “pleating artifact” in the LMCA and Cx artery, induced by the stiff structure of the extra support guidewire, was felt to be likely due to the acute angle of the origin of CX artery from the LMCA. The guide wire was partially withdrawn and the filling defect decreased (Figure 3). A stent was appropriately placed into the in-stent restenosis without any complication. The filling defect completely disappeared after complete withdrawal of the guide wire (Figure 4).
Discussion
“Pleating artifact” is a benign pathology rarely seen during coronary interventions. It can occur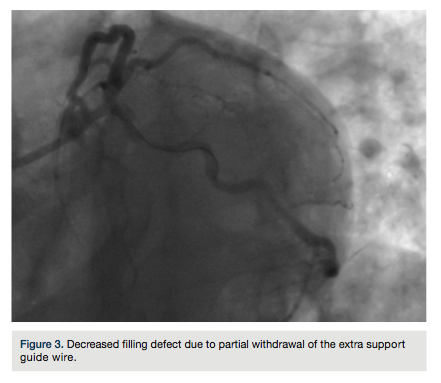 when a curved artery is straightened by a stiff guide wire. Several features of this benign pathology discriminate it from real pathology. It may occur in the irrelevant segment of the vessel, is refractory to nitroglycerin, and resolves when the guide wire is partially or completely withdrawn. It should be distinguished from coronary spasm, dissection, or true stenosis in order to avoid unnecessary stenting or surgery.
when a curved artery is straightened by a stiff guide wire. Several features of this benign pathology discriminate it from real pathology. It may occur in the irrelevant segment of the vessel, is refractory to nitroglycerin, and resolves when the guide wire is partially or completely withdrawn. It should be distinguished from coronary spasm, dissection, or true stenosis in order to avoid unnecessary stenting or surgery.
This article received a double-blind peer review from members of the Cath Lab Digest editorial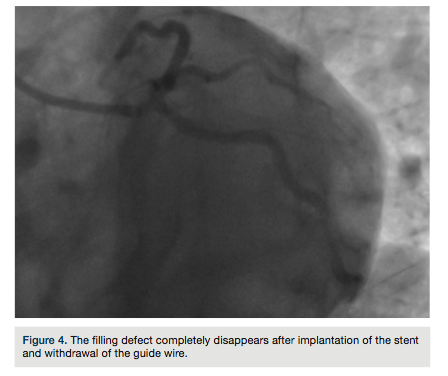 board.
board.
The authors may be contacted via Dr. Aleks Degirmencioglu at alexdegirmencioglu@hotmail.com.
___________________
*Department of Cardiology, Acibadem University Faculty of Medicine, Istanbul, Turkey; †Department of Cardiology, Acibadem Maslak Hospital, Istanbul, Turkey


