


Management of Spontaneous Coronary Artery Dissection Causing an Acute Myocardial Infarction in a Young Female
Introduction
Spontaneous coronary artery dissection (SCAD) is a rarely reported cause of myocardial infarction and sudden cardiac death.1,2 The first case was described by Pretty in 1931.3 Overall incidence of SCAD on coronary angiography is around 0.2%.4
The mean age of presentation is 42 years and 70% of cases are reported in women, of which, 30% were noted either during the third trimester of pregnancy or in the early postpartum period.5 The left anterior descending coronary artery (LAD) is the most commonly affected.1
SCAD may be the result of an intimal rupture, with subsequent disruption of the vessel wall leading to a double lumen. Alternatively, bleeding of the vasa vasorum may result in an intramural hematoma.
The etiology of spontaneous coronary artery dissection remains unclear. Coronary atherosclerosis and the peripartum period are most commonly associated with the development of SCAD. Other predisposing factors have been reported, including hypertension, connective tissue disorders (Marfan’s syndrome, Ehlers-Danlos syndrome), vasculitis (for example, polyarteritis nodosa, systemic lupus erythematosus and eosinophilic arteritis), antiphospholipid antibody syndrome, and inflammatory bowel disease.6 Herein, we describe a complex case of an idiopathic SCAD in a 42-year-old woman, without any related risk factors.
Case presentation
A 42-year-old menstruating woman, without any cardiovascular risk factors or drug abuse,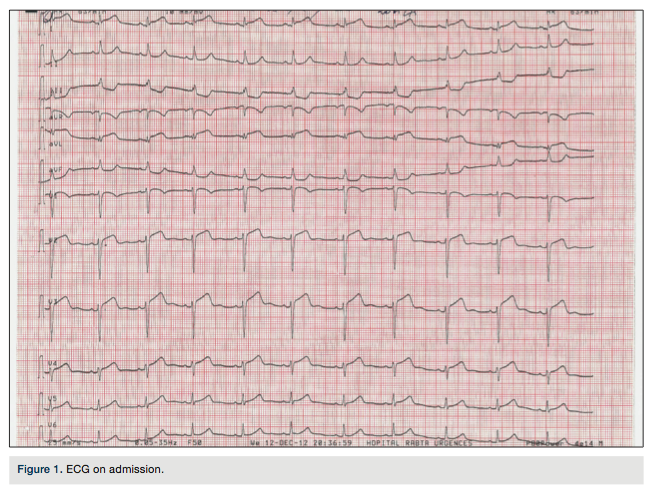 presented to the emergency department with a 6-hour history of chest pain. She referred no prior medical history. The pain was associated with nausea and diaphoresis. In the emergency department, her blood pressure was 130/70 mm Hg, pulse was 75 beats/min, respirations were 22 and there were no signs of heart failure. An electrocardiogram on admission (Figure 1) showed ST-segment elevation in leads V1 through V5, I and aVL, and there was a reciprocal ST-segment depression in leads III and aVF.
presented to the emergency department with a 6-hour history of chest pain. She referred no prior medical history. The pain was associated with nausea and diaphoresis. In the emergency department, her blood pressure was 130/70 mm Hg, pulse was 75 beats/min, respirations were 22 and there were no signs of heart failure. An electrocardiogram on admission (Figure 1) showed ST-segment elevation in leads V1 through V5, I and aVL, and there was a reciprocal ST-segment depression in leads III and aVF.
The patient was treated with aspirin, heparin, intravenous nitroglycerin, and a 600 mg loading dose of clopidogrel, and was referred to our department for urgent angiography.
The coronary angiogram, performed using the right radial approach, revealed a long dissection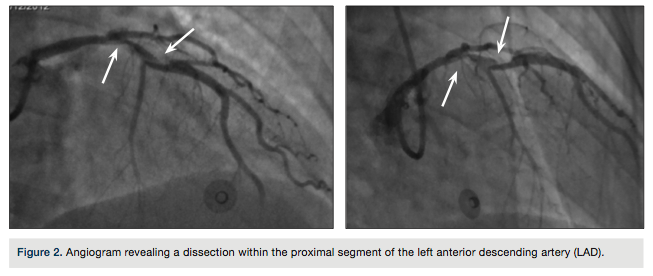 of the proximal tract of the left anterior descending (LAD) artery (TIMI flow II) (Figure 2).
of the proximal tract of the left anterior descending (LAD) artery (TIMI flow II) (Figure 2).
The operator administered intracoronary nitrate and glycoprotein IIb/IIIa inhibitors. Due to the regression of angina with stable hemodynamic parameters, no further operation was performed and the woman was transferred, asymptomatic, to the intensive care unit (ICU).
In the absence of ongoing ischemia, our patient was managed medically. Maximum CPK level was 1906U/l. A full panel of tests, including erythrocyte sedimentation rate, C- reactive protein level, complement level, anti-nuclear antibody test, rheumatoid factor level, perinuclear anti-neutrophil cytoplasmic antibody and centrally accentuated anti-neutrophil cytoplasmic antibody tests, were found to be normal. Our patient was taking oral contraceptives. Echocardiography revealed an apical akinesia with an ejection fraction of 45%.
To provide a better anatomic definition of the dissection, coronary CT angiography was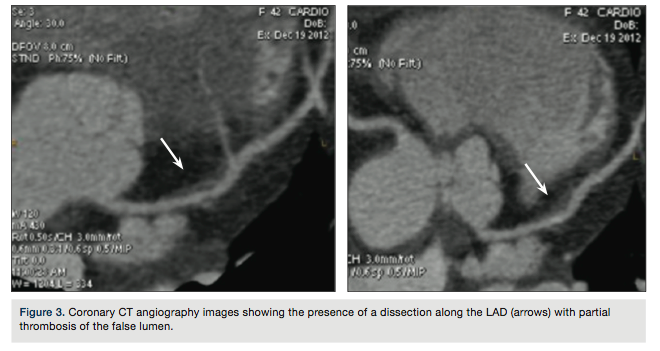 performed 7 days after admission (Figure 3) showing the presence of a dissection along the LAD (arrows) with partial thrombosis of the false lumen. At this point, the patient was discharged.
performed 7 days after admission (Figure 3) showing the presence of a dissection along the LAD (arrows) with partial thrombosis of the false lumen. At this point, the patient was discharged.
The control angiogram, performed 2 months later, showed normal patency of all coronary arteries without any line of dissection (Figure 4) and the echocardiogram demonstrated an ejection fraction of 50% with residual akinesia of the apex.
Discussion
Spontaneous coronary artery dissection (SCAD) is a very rare disease with an incidence of 0.2%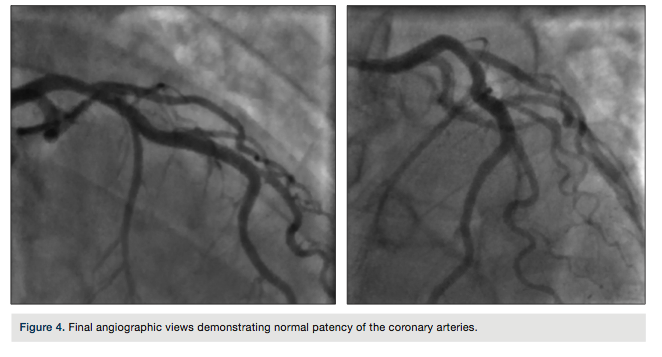 among patients who undergo coronary angiography.4 It should be suspected in healthy middle-aged patients without risk factors for coronary artery disease presenting with an acute chest pain. There are no defined pathways in the management of SCAD, which remains highly controversial. In particular, the value of specific medical regimens or coronary revascularization over a conservative medical management remains unsettled.6,7 The choice is between medical therapy, percutaneous coronary intervention to seal the dissection, or coronary artery bypass graft surgery. A conservative strategy has been found to provide excellent long-term prognosis.8 In the absence of clinical trials and guidelines, treatment decisions continue to be a challenge. For patients presenting with an acute coronary syndrome, initial medical therapy should include antiplatelet and anti-ischemic agents, along with anticoagulation with heparin.9
among patients who undergo coronary angiography.4 It should be suspected in healthy middle-aged patients without risk factors for coronary artery disease presenting with an acute chest pain. There are no defined pathways in the management of SCAD, which remains highly controversial. In particular, the value of specific medical regimens or coronary revascularization over a conservative medical management remains unsettled.6,7 The choice is between medical therapy, percutaneous coronary intervention to seal the dissection, or coronary artery bypass graft surgery. A conservative strategy has been found to provide excellent long-term prognosis.8 In the absence of clinical trials and guidelines, treatment decisions continue to be a challenge. For patients presenting with an acute coronary syndrome, initial medical therapy should include antiplatelet and anti-ischemic agents, along with anticoagulation with heparin.9
Thrombolytic therapy might lyse the thrombus of the false lumen to release the pressure effect of the thrombus on the true lumen. On the other hand, it may increase the flow in the false lumen and cause the dissection to propagate. Thrombolysis has been performed in a few cases with success, but there are also reports of extension of the dissection and worsening of the clinical condition with the administration of thrombolytic agents.10-12 Thus, if the suspicion of coronary artery dissection is high, fibrinolytics should be avoided.
The decision to treat medically or perform percutaneous intervention or surgery must be individualized based on both clinical and angiographic factors. Dissection of large coronary arteries causing persistent ischemia is usually treated with percutaneous intervention or surgery, while dissections of small vessels are treated medically.
Percutaneous intervention with stenting can restore flow in the true lumen, relieving ischemia, and seal the dissection, preventing further expansion. Intravascular ultrasound (IVUS) can aid in diagnosis, particularly when an angiographic intimal flap is not evident. IVUS can be used to confirm guide wire placement in the true lumen, evaluate the length of dissection and vessel size, and assess stent apposition and sealing of the dissection.13 The clinical success rate of stenting in patients with SCAD is over 90%.14 Single-vessel dissections are usually treated with percutaneous intervention with stenting, while left main dissection, multivessel involvement, or failure of percutaneous interventional procedures may require surgical intervention.15 Glycoprotein IIb/IIIa inhibitors may be used as adjunctive therapy during percutaneous intervention for unstable dissections; however, there is a theoretical risk of hematoma expansion with these agents and more data are needed.16
After the resolution of the acute phase, a search into the etiology of the dissection should be pursued to guide future management. In addition to aspirin and beta blockers, patients with underlying coronary artery disease should receive statins. Patients with SCAD during pregnancy or the peripartum period should be counseled on the increased risk of dissection associated with increasing parity and age.9
Possible late complications include progression of the dissection and formation of pseudoaneurysms.5 Patients should be followed for any symptoms of recurrent ischemia. Stress testing with nuclear perfusion imaging is preferred over coronary angiography as a means of surveillance.9
Conclusion
Spontaneous coronary artery dissection should be considered in any young woman with no risk factors for coronary artery disease and acute myocardial infarction. Given the propensity for extension of dissection with or without mechanical revascularization, and documentation of spontaneous healing, medical therapy remains a rational approach. Depending upon hemodynamic stability, however, it is recognized that therapy must be individualized.
This article received a double-blind peer review from members of the Cath Lab Digest Editorial Board.
The authors may be contacted via Dr. Oueslati Chaker at chaker_wes@yahoo.fr.
References
- DeMaio SJ, Kinsella SH, Silverman ME. Clinical course and long term prognosis of spontaneous coronary artery dissection. Am J Cardiol. 1989; 64: 471-474.
- Fish RD. A 37-year-old women with angina pectoris. Circulation. 1994; 89: 898-908.
- Pretty H. Dissecting aneurysms of coronary artery in woman aged 42: rupture. Br Med J. 1931; 1: 667.
- Maeder M, Ammann P, Angehrn W, Rickli H. Idiopathic spontaneous coronary artery dissection: incidence, diagnosis and treatment. Int J Cardiol. 2005 Jun 8; 101(3): 363-369.
- Sabatine MS, Jaffer FA, Staats PN, Stone JR. Case records of the Massachusetts General Hospital. Case 28–2010. A 32-year-old woman, 3 weeks post partum, with substernal chest pain. N Engl J Med. 2010; 363(12): 1164-1173.
- Jorgensen MB, Aharonian V, Mansukhani P, Mahrer PR. Spontaneous coronary dissection: a cluster of cases with this rare finding. Am Heart J. 1994; 127: 1382-1387.
- Hering D, Piper C, Hohmann C, Schultheiss HP, Horstkotte D. [Prospective study of the incidence, pathogenesis and therapy of spontaneous, by coronary angiography diagnosed coronary artery dissection]. Z Kardiol. 1998; 87: 961-970.
- Alfonso F, Paulo M, Lennie V, et al. Spontaneous coronary artery dissection: long-term follow-up of a large series of patients prospectively managed with a ‘conservative’ therapeutic strategy. JACC Cardiovasc Interv. 2012; 5: 1062-1070.
- Kamran M, Guptan A, Bogal M. Spontaneous coronary artery dissection: case series and review. J Invasive Cardiol. 2008, 20(10): 553-559.
- Madu EC, Kesinski DJ, Wilson WR, Bruket MW, Fraker TD, Ansel GI. Two vessel coronary artery dissection in the peripartum period. Angiology. 1994; 45: 809-816.
- Lee TM, Liau CS. Spontaneous coronary artery dissection in an elderly woman with acute inferior myocardial infarction. Angiology. 1995; 46: 847-851.
- Hanratty CG, McKeown PP, O’Keeffe DB. Coronary stenting in the setting of spontaneous coronary artery dissection. Int J Cardiol. 1998; 67: 197-199.
- Iyisoy A, Celik M, Celik T, Yuksel UC. The role of intravascular ultrasound guidance in the treatment of intramural hematoma probably caused by spontaneous coronary artery dissection in a young woman with acute anterior myocardial infarction. Cardiol J. 2012; 19(5): 532-535.
- Moukarbel GV, Alam SE. Spontaneous coronary artery dissection: management options in the stent era. J Invasive Cardiol. 2004 Jun; 16(6): 333-335
- Kamineni R, Sadhu A, Alpert JS. Spontaneous coronary artery dissection: report of two cases and a 50-year review of the literature. Cardiol Rev. 2002 Sep-Oct; 10(5): 279-284.
- Cheung S, Mithani V, Watson RM. Healing of spontaneous coronary dissection in the context of glycoprotein IIB/IIIA inhibitor therapy: a case report. Catheter Cardiovasc Interv. 2000 Sep; 51(1): 95-100.


