


Endovascular Management of a Left Innominate Vein Chronic Total Occlusion Using an Antegrade-Retrograde Approach
Abstract
Deep venous thrombosis is common and portends a heightened risk for development of post- thrombotic syndrome. Chronic venous occlusions can result in significant morbidity and an increased lifetime burden of medical care. Herein, we present a case of chronic upper extremity venous occlusion with debilitating symptoms that was treated successfully with venoplasty and stenting.
thrombotic syndrome. Chronic venous occlusions can result in significant morbidity and an increased lifetime burden of medical care. Herein, we present a case of chronic upper extremity venous occlusion with debilitating symptoms that was treated successfully with venoplasty and stenting.
Case
A 71-year-old male with a past medical history of chronic kidney disease stage 5, diabetes, and hepatitis C with liver cirrhosis and concomitant thrombocytopenia was transferred to our facility with progressive worsening left upper extremity edema over one year (Figure 1). Previous ultrasound study demonstrated total occlusion of the left innominate vein (IV). The initial attempt at revascularization at the transferring facility was unsuccessful, and the patient was transferred to our facility for repeat attempt at IV intervention.
(Figure 1). Previous ultrasound study demonstrated total occlusion of the left innominate vein (IV). The initial attempt at revascularization at the transferring facility was unsuccessful, and the patient was transferred to our facility for repeat attempt at IV intervention.
Access was obtained in the right femoral vein as well as the left basilic vein with 6 French (Fr) sheaths. Selective venogram of the left basilic vein confirmed occlusion of the left IV at the termination of the left internal jugular vein and the subclavian vein (Figure 2). The right femoral vein sheath was exchanged for a 7 Fr Pinnacle Destination sheath (Terumo) and advanced into the superior vena cava (SVC) to the point of occlusion at the left IV. Selective venogram from the SVC confirmed a proximal occlusion of the left IV (Figure 3). Multiple attempts were made to cross the occlusion from the right femoral vein approach using a stiff-angled Glidewire (Terumo) with a Quick-Cross support catheter (Spectranetics), but we were unable to enter the true lumen of the left IV. We advanced the Glidewire with the stiffer, back end of the wire in an attempt to cross the fibrotic chronic occlusion from the SVC, which partially crossed the occlusion, but entered a dissection plane in the left IV. The Glidewire was advanced from the left
advanced into the superior vena cava (SVC) to the point of occlusion at the left IV. Selective venogram from the SVC confirmed a proximal occlusion of the left IV (Figure 3). Multiple attempts were made to cross the occlusion from the right femoral vein approach using a stiff-angled Glidewire (Terumo) with a Quick-Cross support catheter (Spectranetics), but we were unable to enter the true lumen of the left IV. We advanced the Glidewire with the stiffer, back end of the wire in an attempt to cross the fibrotic chronic occlusion from the SVC, which partially crossed the occlusion, but entered a dissection plane in the left IV. The Glidewire was advanced from the left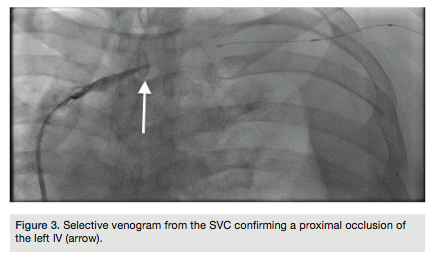 basilic vein access site, but again, we were unable to enter the true lumen in the SVC. The stiffer back end of the Glidewire was advanced via the left basilic vein access, which successfully crossed through the occlusion of the IV into the true lumen in the SVC. The Quick-Cross support catheter was then advanced over the Glidewire into the SVC. Selective venogram through the catheter confirmed intraluminal position in the SVC. A 25-mm GooseNeck snare (Covidien) advanced from the right femoral vein access was used to retrieve the wire from the left basilic vein access to form a rail between both access sites. Serial balloon venoplasty was performed with a 4.0 x 100 mm Mustang balloon (Boston Scientific), 6.0 x 100 mm Mustang
basilic vein access site, but again, we were unable to enter the true lumen in the SVC. The stiffer back end of the Glidewire was advanced via the left basilic vein access, which successfully crossed through the occlusion of the IV into the true lumen in the SVC. The Quick-Cross support catheter was then advanced over the Glidewire into the SVC. Selective venogram through the catheter confirmed intraluminal position in the SVC. A 25-mm GooseNeck snare (Covidien) advanced from the right femoral vein access was used to retrieve the wire from the left basilic vein access to form a rail between both access sites. Serial balloon venoplasty was performed with a 4.0 x 100 mm Mustang balloon (Boston Scientific), 6.0 x 100 mm Mustang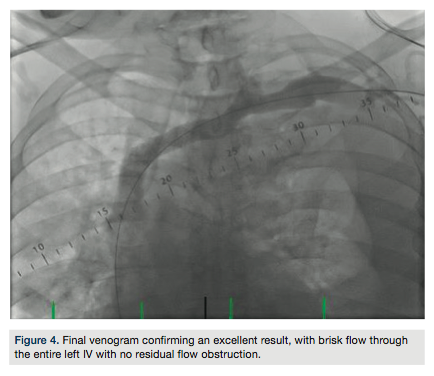 balloon, and then a 10.0 x 60 mm Mustang balloon, with good expansion. A Protégé 14 x 80 mm self-expanding stent (Covidien) was then deployed in the left IV and post-dilated with a 12.0 x 40 mm Mustang balloon. Final venogram confirmed an excellent result, with brisk flow through the entire left IV and no residual flow obstruction (Figure 4). Intravascular ultrasound imaging of the stented segment confirmed adequate stent apposition and expansion (Figure 5). Hemostasis was achieved in bilateral access sites with manual compression and the left upper extremity wrapped in compression bandages (Figure 6). The patient was subsequently transferred back to the original facility for management of his post-procedural care.
balloon, and then a 10.0 x 60 mm Mustang balloon, with good expansion. A Protégé 14 x 80 mm self-expanding stent (Covidien) was then deployed in the left IV and post-dilated with a 12.0 x 40 mm Mustang balloon. Final venogram confirmed an excellent result, with brisk flow through the entire left IV and no residual flow obstruction (Figure 4). Intravascular ultrasound imaging of the stented segment confirmed adequate stent apposition and expansion (Figure 5). Hemostasis was achieved in bilateral access sites with manual compression and the left upper extremity wrapped in compression bandages (Figure 6). The patient was subsequently transferred back to the original facility for management of his post-procedural care.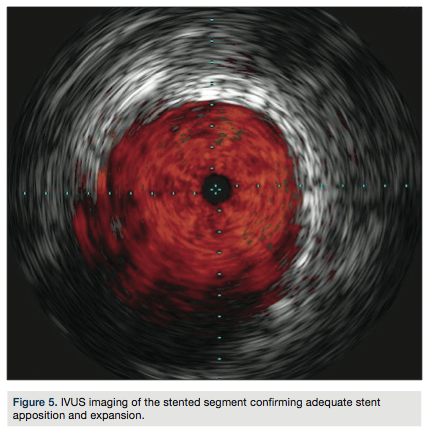
Discussion
Venous thrombosis occurs in approximately 1 in every 1,000 persons per year.1 Of patients with confirmed deep vein thrombosis (DVT), 11% had an upper extremity DVT, which usually refers to thrombosis of the axillary or subclavian veins. Significant risk factors for upper extremity DVT include placement of a central venous catheter, pacemaker and malignancy.2 Although anticoagulation effectively prevents thrombus extension, pulmonary embolism, death, and recurrence3, follow-up studies of patients with DVT who were treated with anticoagulants have shown that in most cases, only partial clearance of thrombus occurs and return of normal physiological function of the vein is rare.4 Many patients develop venous dysfunction and valvular incompetence resulting in post-thrombotic syndrome (PTS), often characterized by pain, swelling, heaviness, edema, cramps, pigmentation, skin breakdown, and even ulceration.5 PTS is associated with reduced individual quality of life and increased cost of health care.6
clearance of thrombus occurs and return of normal physiological function of the vein is rare.4 Many patients develop venous dysfunction and valvular incompetence resulting in post-thrombotic syndrome (PTS), often characterized by pain, swelling, heaviness, edema, cramps, pigmentation, skin breakdown, and even ulceration.5 PTS is associated with reduced individual quality of life and increased cost of health care.6
There is increasing evidence that early recognition and invasive treatment of DVT can reduce the incidence of PTS. As many as 82% of patients will develop PTS after a single episode of DVT.7 In the acute setting of lower extremity DVT, catheter-directed thrombolysis has been shown to be efficacious with low risk of bleeding for patients.8 Pharmacomechanical thrombectomy offers a safe and effective alternative for treatment of acute DVT7, although limited by age of clot when greater than three days old.9 Chronic DVT results in inflammatory changes leading to vein wall fibrosis and chronic occlusion with outflow obstruction. Endovascular treatment, in the form of angioplasty and stenting, has been shown to relieve symptoms and improve quality of life.10-11
In a study of 870 patients with 982 chronic nonmalignant obstructive lesions of the iliocaval veins that were stented, there was no incidence of 30-day mortality. At 72-month follow-up, cumulative primary, primary-assisted, and secondary patency rates were 57%, 80%, and 86% for post-thrombotic obstructions, respectively.12 Thus, endovenous angioplasty combined with stenting is a safe and effective treatment strategy, with good long-term patency rates.
We present herein a case of left IV chronic occlusion intervention via an antegrade-retrograde approach with successful venoplasty and stenting.
Disclosure: Drs. Hakimi, Ghods and Giri report no conflicts of interest regarding the content herein. Dr. George reports that he is a consultant for Boston Scientific and Covidien.
Jon C. George, MD, can be contacted at jcgeorgemd@gmail.com.
References
- White RH. The epidemiology of venous thromboembolism. Circulation. 2003; 107: I4-l8.
- Joffe HV, Kucher N, Tapson VF, Goldhaber SZ; Deep Vein Thrombosis (DVT) FREE Steering Committee. Upper-extremity deep vein thrombosis: A prospective registry of 592 patients. Circulation. 2004; 110: 1605-1611.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ; American College of Chest Physicians. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008; 133(6 Suppl): 454S-545S.
- Piovella F, Crippa L, Barone M, Viganò D’Angelo S, Serafini S, Galli L, Beltrametti C, D’Angelo A. Normalization rates of compression ultrasonography in patients with a first episode of deep vein thrombosis of the lower limbs: association with recurrence and new thrombosis. Haematologica. 2002; 87: 515-522.
- Kahn SR. The post-thrombotic syndrome: progress and pitfalls. Br J Haematol. 2006; 134(4): 357-365.
- Kahn SR, Hirsch A, Shrier I. Effect of postthrombotic syndrome on health-related quality of life after deep venous thrombosis. Arch Intern Med. 2002; 162(10): 1144-1148.
- Titus JM, Moise MA, Bena J, Lyden SP, Clair DG. Iliofemoral stenting for venous occlusive disease. J Vasc Surg. 2011; 53: 706-712.
- Enden T, Haig Y, Kløw NE, Slagsvold CE, Sandvik L, Ghanima W, et al; CaVenT Study Group. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. 2012; 379(9810): 31-38.
- Rao AS, Konig G, Leers SA, Cho J, Rhee RY, Makaroun MS, Chaer RA. Pharmacomechanical thrombectomy for iliofemoral deep vein thrombosis: an alternative in patients with contraindications to thrombolysis. J Vasc Surg. 2009; 50(5): 1092-1098.
- Hartung O, Otero A, Boufi M, De Caridi G, Barthelemy P, Juhan C, Alimi YS. Mid-term results of endovascular treatment for symptomatic chronic nonmalignant iliocaval venous occlusive disease. J Vasc Surg. 2005; 42: 1138-1144.
- Neglén P, Hollis KC, Olivier J, Raju S. Stenting of the venous outflow in chronic venous disease: long-term stent-related outcome, clinical, and hemodynamic result. J Vasc Surg. 2007; 46(5): 979-990.
- O’Sullivan GJ, Lohan DG, Gough N, Cronin CG, Kee ST. Pharmacomechanical thrombectomy of acute deep vein thrombosis with the Trellis-8 isolated thrombolysis catheter. J Vasc Interv Radiol. 2007; 18(6): 715-724.
________________________
*Division of Interventional Cardiology and Endovascular Medicine, Deborah Heart and Lung Center, Browns Mills, New Jersey, †Penn Heart and Vascular Center, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania


