


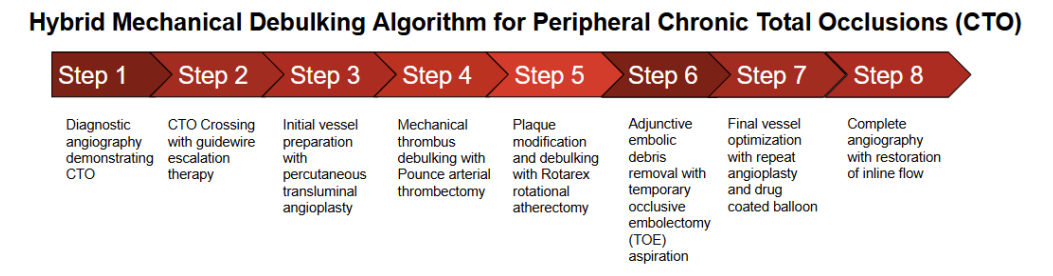
Combined Rotational Atherectomy and Mechanical Thrombectomy for Debulking of Peripheral Chronic Total Occlusions
A Case Series With Adjunctive Temporary Occlusive Embolectomy
A Case Series With Adjunctive Temporary Occlusive Embolectomy
Key Summary
- In a retrospective single-center case series of 7 symptomatic peripheral arterial disease patients with lower-extremity chronic total occlusions (CTOs), 6 out of 7 had 100% in-stent occlusion. Treatment combined mechanical thrombectomy and rotational atherectomy with adjunctive temporary occlusive embolectomy aspiration.
- Technical success was 100%, with restoration of inline flow in all cases. No distal embolization events and no major procedural complications were reported. Procedural success was observed regardless of whether thrombectomy or atherectomy was performed first.
- Authors conclude the hybrid debulking approach appears feasible and adaptable, particularly for in-stent CTOs, and adjunctive aspiration may help reduce embolic risk. Limitations include small sample size, single-center experience, and no long-term follow-up; larger studies are needed.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT. 2026;23(6):E84-E91
Abstract
Chronic total occlusion (CTO) lesions of the lower extremity arteries remain a challenging subset of peripheral artery disease interventions due to heavy plaque burden, thrombotic components, and frequent occurrence of in-stent occlusion. Effective vessel preparation is essential for successful endovascular revascularization. Objective: To describe the feasibility of a hybrid mechanical debulking strategy combining rotational atherectomy and mechanical thrombectomy for treatment of complex lower extremity CTO lesions. Methods: Seven patients undergoing endovascular treatment of CTO lesions were retrospectively analyzed. Five infrainguinal lesions were treated via contralateral crossover access using sequential vessel preparation with percutaneous transluminal angioplasty, mechanical thrombectomy using the Pounce arterial thrombectomy system (Surmodics), and rotational atherectomy with the Rotarex atherectomy system (BD). The sequence of thrombectomy and atherectomy was performed in variable order depending on operator preference. Following debulking, distal aspiration using a temporary occlusive embolectomy technique was performed to remove embolic debris. Two cases involving iliac to common femoral artery in-stent occlusion were treated using alternative access strategies. Results: Six of seven cases involved complete in-stent occlusion. Successful revascularization with restoration of inline flow was achieved in all cases. No distal embolization or major procedural complications were observed. Comparable procedural success was achieved regardless of the sequence of thrombectomy and atherectomy. Conclusion: Combined mechanical thrombectomy and rotational atherectomy appears to be a feasible and versatile strategy for debulking complex peripheral CTO lesions, particularly in the setting of in-stent occlusion. Device sequencing may be flexible without compromising procedural success. Adjunctive distal aspiration may help mitigate embolic risk following aggressive plaque modification.
Introduction
Peripheral artery disease (PAD) affects more than 200 million individuals worldwide and is associated with significant morbidity due to claudication and chronic limb-threatening ischemia.1,2 Chronic total occlusion (CTO) lesions of the lower extremity arteries are frequently encountered during endovascular interventions and remain among the most technically challenging lesion subsets to treat.3
Contemporary treatment strategies emphasize endovascular revascularization for many femoropopliteal lesions, as reflected in guidelines from the American College of Cardiology and the American Heart Association.1 However, CTO lesions, particularly those involving in-stent restenosis, often contain a complex mixture of fibrocalcific plaque and organized thrombus.4 This heterogeneous composition may limit the effectiveness of conventional balloon angioplasty alone and increase the risk of procedural complications.
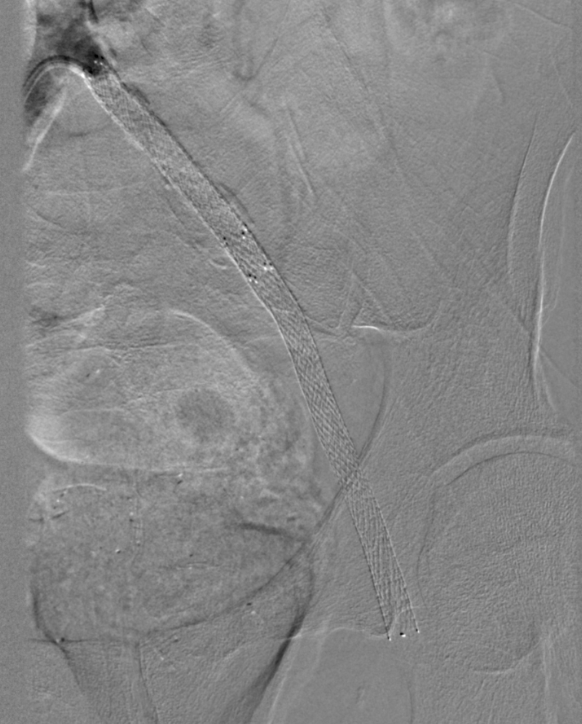
For this reason, vessel preparation strategies involving mechanical debulking have become increasingly important in peripheral interventions.5 Rotational atherectomy using the Rotarex atherectomy system (BD) provides mechanical fragmentation and aspiration of plaque and thrombotic material6 (Figure 1), while mechanical thrombectomy devices such as the Pounce arterial thrombectomy system (Surmodics) enable direct extraction of organized thrombus7(Figure 2). These devices have traditionally been used independently, depending on the dominant lesion component. However, many CTO lesions—particularly those occurring within previously implanted stents—contain both thrombotic and atherosclerotic elements,4 suggesting that a combined debulking strategy may be advantageous.
Despite the theoretical synergy of these approaches, there are limited reports describing the sequential use of thrombectomy and rotational atherectomy for treatment of peripheral CTO lesions.
In this report, we describe a series of patients undergoing endovascular treatment of complex lower extremity CTO lesions using a hybrid debulking strategy combining mechanical thrombectomy and rotational atherectomy, with adjunctive distal aspiration using a temporary occlusive embolectomy technique to remove embolic debris (Figure 3).


This study represents a retrospective case series of seven patients undergoing endovascular treatment for lower extremity chronic total occlusions at a single tertiary center.
Methods
Patient characteristics
Seven patients with symptomatic PAD underwent intervention for CTO lesions (Table).
Table. Case summary.
| Case | Lesion location | In-stent | Access | Devices Used | Outcome |
| 1 | Popliteal | Yes | Contralateral CFA | PTA + Pounce + Rotarex + TOE |
Success |
| 2 | Popliteal/SFA | No | Contralateral CFA | PTA + Pounce + Rotarex + TOE | Success |
| 3 | SFA | Yes | Contralateral CFA | PTA + Pounce + Rotarex + TOE | Success |
| 4 | SFA | Yes | Contralateral CFA | PTA + Pounce + Rotarex + TOE | Success |
| 5 | Common iliac to SFA | Yes | Ipsilateral CFA | Rotarex + Pounce + PTA | Success |
| 6 | SFA | Yes | Contralateral CFA | PTA + Pounce + Rotarex + TOE | Success |
| 7 | Common Iliac to CFA | Yes | Contralateral CFA | PTA + Pounce + Rotarex + TOE | Success |
Abbreviations: CFA, common femoral artery; PTA, percutaneous transluminal angioplasty; TOE, temporary occlusive embolectomy; SFA, superficial femoral artery.
Key characteristics:
- Six of seven cases involved 100% in-stent occlusion
- Five lesions were infrainguinal below the iliac arteries
- Two lesions involved in-stent occlusion extending from the common iliac artery to the common femoral artery
Endovascular procedure
Infrainguinal chronic total occlusion technique (5 cases)
Five patients with infrainguinal CTO lesions were treated via contralateral common femoral artery access with crossover approach.
After lesion crossing, a hybrid debulking strategy was utilized consisting of:
- Initial vessel preparation with percutaneous transluminal angioplasty
- Mechanical thrombectomy using the Pounce arterial thrombectomy system7
- Rotational atherectomy using the Rotarex atherectomy system6
The sequence of thrombectomy and atherectomy was variable, with some cases utilizing thrombectomy prior to atherectomy and others utilizing atherectomy first, based on operator assessment of lesion composition.
Temporary occlusive embolectomy technique
The temporary occlusive embolectomy (TOE) technique was performed to reduce the risk of distal embolization following mechanical debulking.
This technique involved:
- Placement of a blood pressure cuff at the infrapopliteal segment
- Inflation to temporarily occlude distal arterial flow
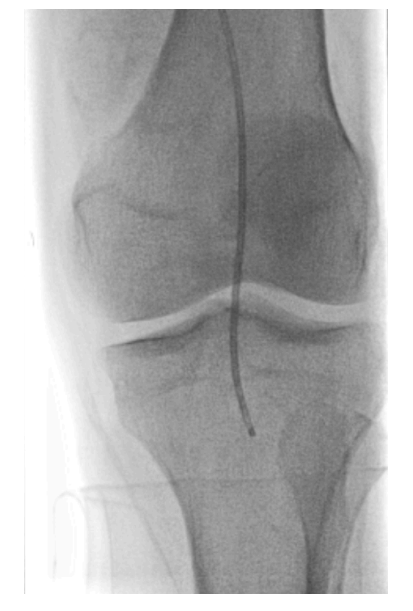
A long 6F multipurpose catheter was advanced to the distal popliteal artery (Figure 4). Manual aspiration thrombectomy was then performed using a 20-cc syringe, aspirating proximally through the superficial femoral artery to remove debris generated during intervention. The cuff was then deflated, followed by completion angiography confirming restoration of inline flow.
Iliac–common femoral artery in-stent occlusion cases (2 cases)
Two patients presented with 100% in-stent occlusion extending from the common iliac artery to the common femoral artery (CFA).4
- One case utilized ipsilateral retrograde CFA access
- One case utilized contralateral crossover approach
Both cases were treated using combinations of:
- Rotarex atherectomy system6
- Pounce arterial thrombectomy system7
- Percutaneous transluminal angioplasty
with variable sequencing of thrombectomy and atherectomy, demonstrating procedural flexibility.
Results
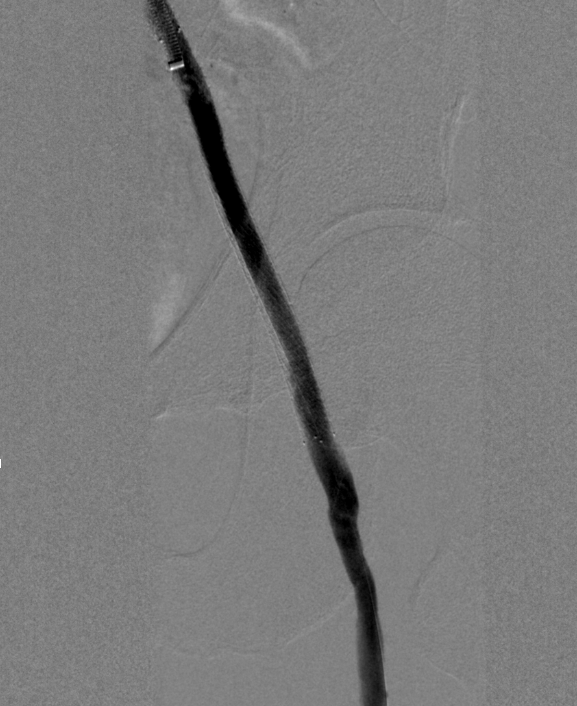
The sequential hybrid debulking approach with adjunctive distal aspiration resulted in:
- 100% technical success
- Restoration of inline flow in all cases
- No distal embolization events
- No major procedural complications
Importantly, successful outcomes were achieved regardless of whether thrombectomy or atherectomy was performed first, suggesting that the hybrid approach is adaptable to lesion characteristics.
Discussion
Hybrid mechanical debulking strategy
The primary innovation described in this case series is the combined use of mechanical thrombectomy and rotational atherectomy for treatment of complex peripheral CTO lesions (Figures 5 and 6). Mechanical thrombectomy using the Pounce arterial thrombectomy system allows extraction of organized thrombus,7 while rotational atherectomy using the Rotarex atherectomy system facilitates fragmentation and aspiration of residual plaque.6
Flexibility of device sequencing
An important observation from this series is that the sequence of thrombectomy and atherectomy may be interchangeable without compromising procedural success. In several cases, thrombectomy was performed prior to atherectomy to remove bulk thrombus. In others, atherectomy was performed first to modify plaque and facilitate subsequent thrombus extraction. This suggests that:
- Lesion-specific strategy can guide sequencing
- Operators may tailor approach based on thrombus vs plaque burden
- Hybrid debulking remains effective regardless of sequence
This flexibility may be particularly relevant in in-stent occlusion, where lesion composition is heterogeneous.4
Role of adjunctive temporary occlusive embolectomy technique
Aggressive debulking carries risk of distal embolization. The TOE aspiration technique was used as an adjunct to remove embolic debris (Figure 7). While not the primary innovation, it represents a simple, low-cost adjunct that may enhance procedural safety.
Clinical relevance
Six of seven cases involved complete in-stent occlusion, a high-risk lesion subset.4 The consistent success observed in this cohort highlights the potential role of hybrid debulking strategies in complex restenotic disease.
Limitations
This study is limited by:
- Small sample size
- Single-center experience
- Lack of long-term follow-up
Conclusions
Combined mechanical thrombectomy and rotational atherectomy represents a feasible, effective, and adaptable strategy for treatment of complex peripheral CTO lesions. Device sequencing may be flexible without compromising outcomes, and adjunctive distal aspiration may further enhance procedural safety.
Affiliations and Disclosures
From Henry Ford Warren Hospital, Warren, Michigan.
The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted June 4, 2026.
Address for correspondence: Fares Jamal, 3275 Bloomfield Shore Dr., West Bloomfield, MI 48323. Email: faresjamal1@gmail.com
References
1. Writing Committee Members; Gornik HL, Aronow HD, Goodney PP, et al. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS guideline for the management of lower extremity peripheral artery disease. J Am Coll Cardiol. 2024;83(24):2497-2604 doi:10.1016/j.jacc.2024.02.013
2. Fowkes FGR, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901):1329-1340. doi:10.1016/S0140-6736(13)61249-0
3. Tsai S, Liu Y, Hoang L, et al. Comparative outcomes of interventions for femoropopliteal chronic total occlusion versus non-chronic total occlusion lesions from the multicenter XLPAD registry. J Am Heart Assoc. 2023;12(12):e028425. doi:10.1161/JAHA.122.028425
4. Tosaka A, Soga Y, Iida O, et al. Classification and clinical impact of restenosis after femoropopliteal stenting. J Am Coll Cardiol. 2012;59(1):16-23. doi:10.1016/j.jacc.2011.09.036
5. Ormiston W, Dyer-Hartnett S, Fernando R, Holden A. An update on vessel preparation in lower limb arterial intervention. CVIR Endovasc. 2020;3(1):86. doi:10.1186/s42155-020-00175-6
6. Loffroy R, Edriss N, Goyault G, et al. Percutaneous mechanical atherothrombectomy using the Rotarex®S device in peripheral artery in-stent restenosis or occlusion: a French retrospective multicenter study on 128 patients. Quant Imaging Med Surg. 2020;10(1):283-293. doi:10.21037/qims.2019.11.15
7. Gray BH, Wheibe E, Dicks AB, Low ML, Tingen JS. Pounce thrombectomy system to treat acute and chronic peripheral arterial occlusions. Ann Vasc Surg. 2023;96:104-114. doi:10.1016/j.avsg.2023.05.019

