Atypical Pityriasis Rosea
Pityriasis rosea, sometimes referred to as pityriasis circinata, roseola annulata, or herpes tonsurans maculosus, is an acute papulosquamous eruption that typically resolves on its own. Although its exact etiology remains unclear, epidemiologic features, such as seasonality and case clustering, suggest an infectious trigger. Proposed associations include viral, bacterial, and spirochetal infections, as well as noninfectious factors, such as atopy and autoimmune mechanisms.1,2 In particular, reactivation of latent human herpesvirus 6 and 7 has emerged as the most widely supported hypothesis.1,3,4
Case Report
A 35-year-old man presented with a 1-month history of erythematous, scaly plaques localized to the face and neck. The eruption developed suddenly without fever, arthralgias, sore throat, or other systemic symptoms. He denied new medications and reported no recent use of new topical products. Pruritus was absent to mild.
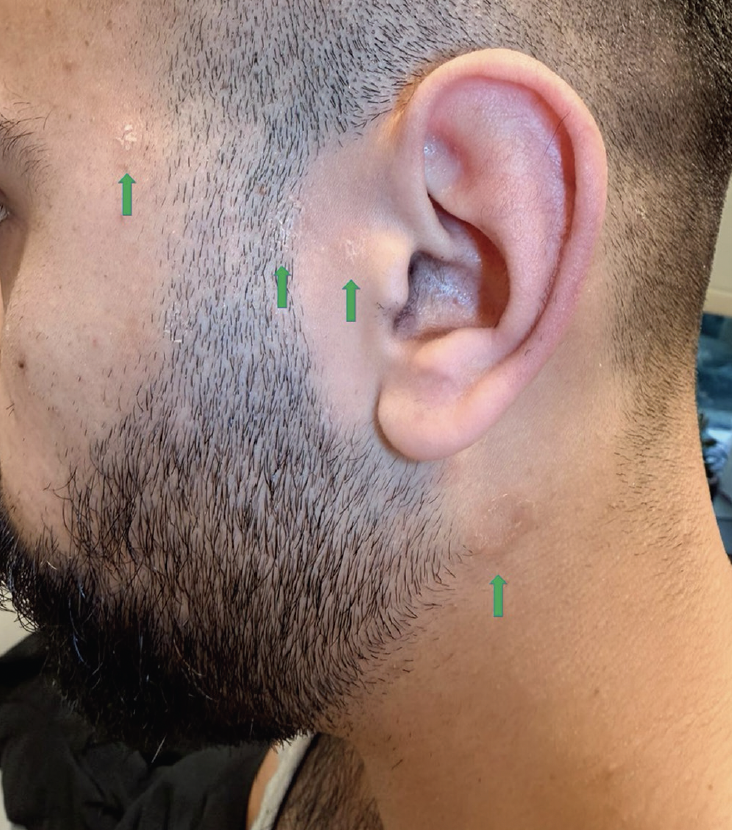
On examination, there were several well-demarcated erythematous plaques with fine scale involving the left temporal hairline, left preauricular region, and left neck. Scale was most appreciable at the periphery on close inspection (Figure 1). No mucosal lesions, palmoplantar involvement, or nail dystrophy was observed. Cervical lymphadenopathy was not present. A punch biopsy was performed for definitive diagnosis.
A full skin examination demonstrated additional ovoid erythematous, scaly plaques on the trunk oriented along cleavage lines (Figure 2). The patient reported that it first started on his trunk as a relatively larger plaque and, over the following days, subsequently spread to other body sites.
Laboratory tests were unremarkable, including negative serologic testing for syphilis (VDRL) and direct fungal examination (KOH preparation), helping exclude key infectious mimickers.
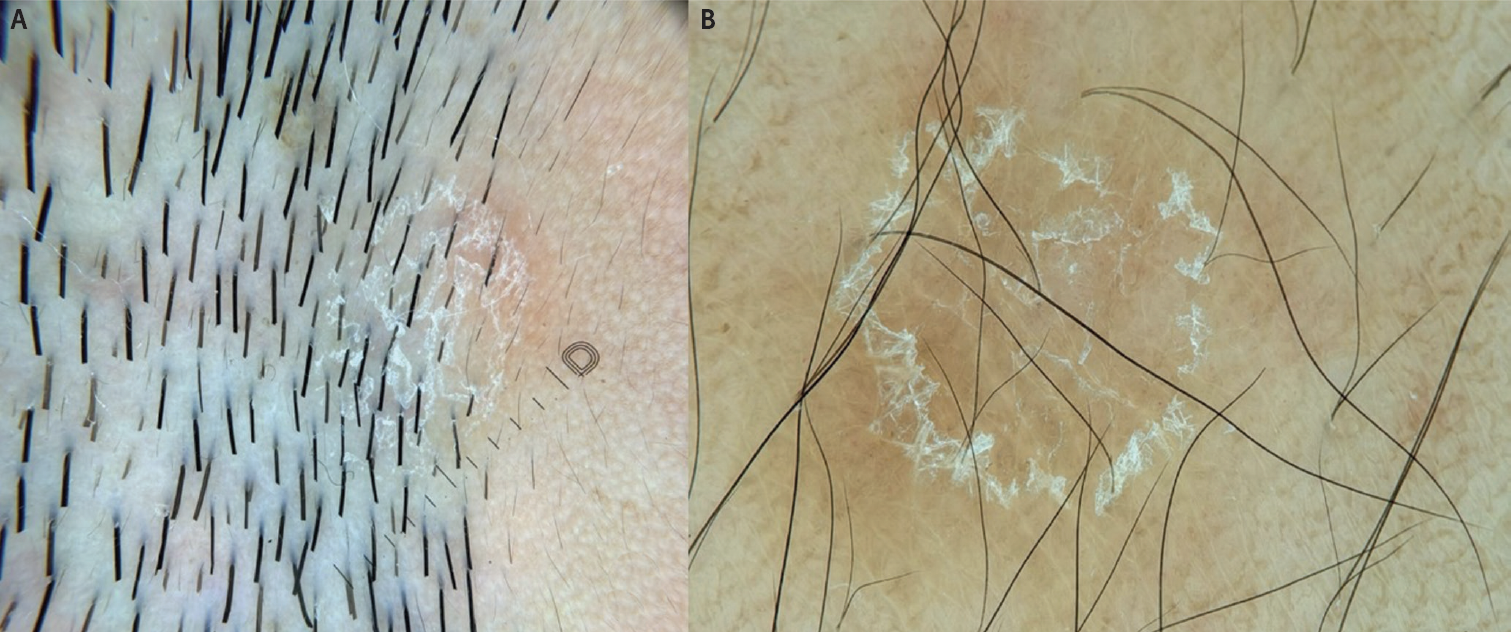
Dermoscopy demonstrated a peripheral collarette of scale on a diffuse erythematous-brown background (Figure 3).
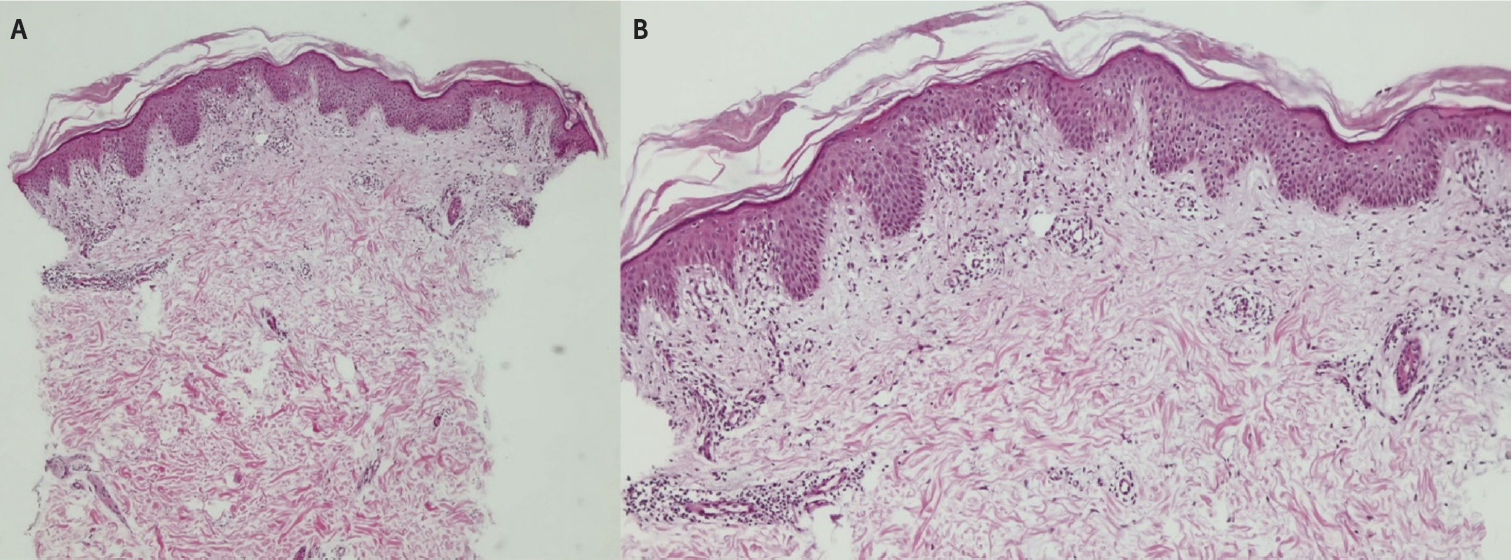
Histopathologic examination revealed partial loss of the granular layer, focal parakeratosis, epidermal spongiosis with lymphocytic exocytosis, a superficial perivascular lymphohistiocytic infiltrate, and vacuolar alteration of the basal layer (Figure 4).
Overall, the clinical, laboratory, dermoscopic, and histopathologic findings supported the diagnosis of pityriasis rosea.
Clinical Presentation

Pityriasis rosea typically presents as an acute papulosquamous eruption with a biphasic course, beginning with a herald patch in approximately 80% of cases, followed 4 to 14 days later by multiple smaller, oval plaques on the trunk and proximal extremities. Lesions are dull pink to salmon-colored with a fine peripheral collarette of scale and are often oriented along Langer lines, producing characteristic “Christmas tree” or V-shaped patterns.2,3,5 Pruritus is variable, with significant itching reported in about one-quarter of patients, while mild prodromal symptoms occur in roughly 5%.4
Pityriasis rosea most commonly affects individuals aged 10 to 35 years, has an estimated incidence of 0.5% to 2%, and appears more frequently in women.4,6,7 Facial and cervical involvement is uncommon and seen mainly in children.4,8,9 Atypical variants account for approximately 20% of cases and include diverse morphologic and distributional patterns.4,10 The disease is benign and self-limited, resolving spontaneously within 6 to 10 weeks,2,5 with rare recurrence (< 5%) and infrequent complications.4,11
Dermoscopy
Dermoscopy can provide supportive pattern recognition in pityriasis rosea, particularly when anatomic distribution is atypical. Most reported dermoscopic patterns include peripheral collarette scale (often the most consistent clue), a diffuse red background, loosely arranged dotted vessels that tend to be peripheral/patchy distributed, variable yellowish hues, and occasional brown globules depending on lesion age and skin phototype.12,13
Histopathology
Histopathologic findings in pityriasis rosea are generally nonspecific and overlap with chronic dermatitis; therefore, clinicopathologic correlation is essential. Typical biopsy features include partial loss of the granular layer and focal, often angulated, parakeratosis, historically described as “teapot” or “tea-kettle” parakeratosis, corresponding to the characteristic peripheral collarette of scale.14 Additional findings may include mild spongiosis with variable lymphocytic exocytosis, superficial perivascular lymphohistiocytic infiltrate, extravasated erythrocytes in the papillary dermis, basal vacuolar change, dyskeratosis, papillary dermal collagen homogenization, and occasional intraepidermal vesicles.2,4
A confluent lichenoid/interface infiltrate is not typical of pityriasis rosea and should prompt consideration of pityriasis lichenoides, drug eruption, or early mycosis fungoides, depending on the clinical context.
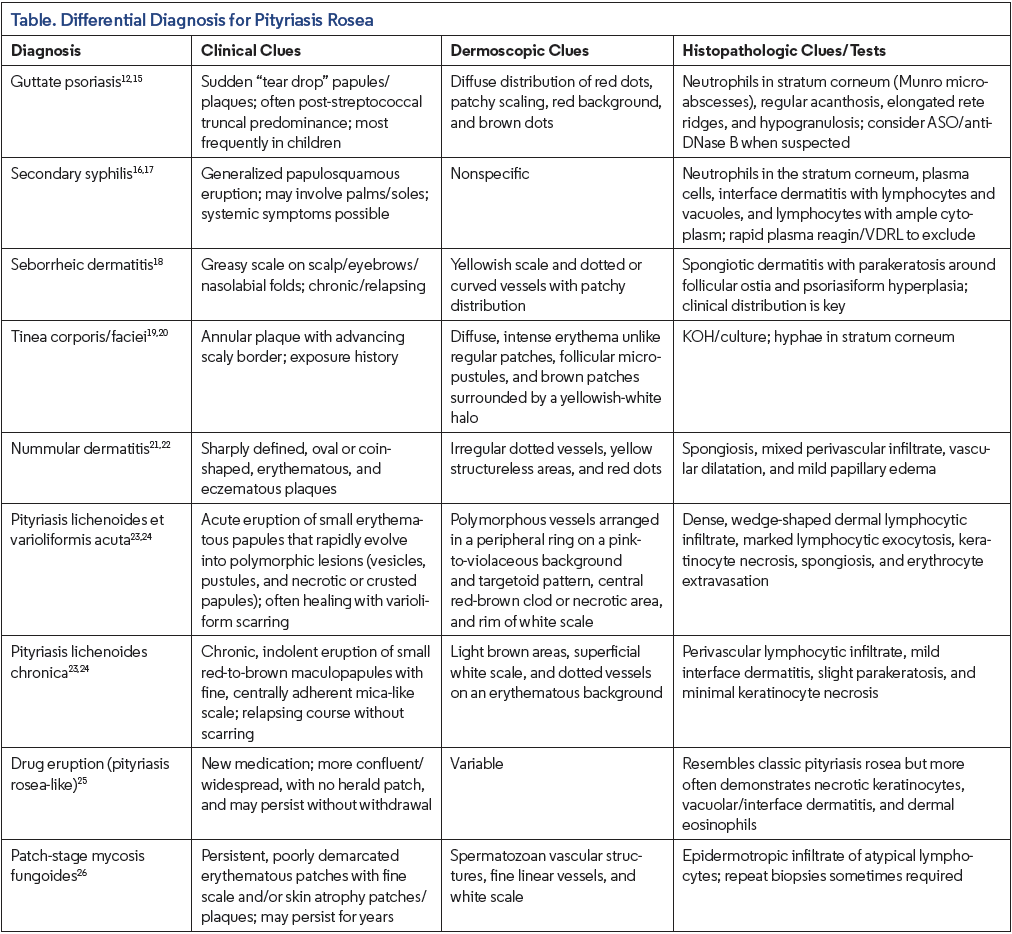
Differential Diagnosis
When pityriasis rosea presents on the face/neck, the differential broadens (Table).15-26 In a patient with facial or cervical papulosquamous plaques, it is essential to exclude infectious causes, including dermatophytosis and secondary syphilis, before considering other differential diagnoses. It is reasonable to obtain KOH and VDRL serology early. If these are negative and the eruption is otherwise compatible, initial symptomatic treatment and observation are appropriate, with biopsy reserved for persistent, progressive, or diagnostically discordant cases.1 In our patient, a biopsy was performed at the initial visit due to significant patient anxiety and a preference for diagnostic confirmation rather than clinical observation.
Management
Pityriasis rosea is typically self-limited; treatment aims to reduce symptoms and avoid unnecessary interventions. Patients should be reassured about the typically benign course and expected resolution. For symptomatic relief, topical corticosteroids and regular emollient use can help reduce erythema and pruritus, with oral antihistamines added as needed for itch. In selected patients with widespread, significantly symptomatic disease, narrowband ultraviolet B therapy may be considered.5,27 If active intervention is needed, there is evidence supporting the use of oral macrolides and acyclovir to shorten the duration of illness.5,28
In this case, diagnostic difficulty arose from involvement of the face and neck, which are atypical sites for classic pityriasis rosea, in conjunction with pre-existing facial findings consistent with seborrheic dermatitis, which could have led to misattribution of newly developed plaques in the same region to a disease flare. However, the identification of truncal lesions aligned along cleavage lines, negative KOH examination and VDRL serology, and the absence of clinical and histopathologic features supporting alternative diagnoses favored pityriasis rosea. Dermoscopic findings along with supportive histopathologic features, including focal parakeratosis with spongiosis and vacuolar alteration of the basal layer, provided further diagnostic corroboration.
The patient was treated with a mid-potency topical corticosteroid and emollients, with complete resolution within 6 weeks, consistent with the expected self-limited course.
Conclusion
Pityriasis rosea should remain on the differential for papulosquamous eruptions even when distribution is atypical, including face/neck-predominant disease. A complete skin examination is essential to identify supportive truncal morphology and distribution. Dermoscopy and histopathology can be valuable adjuncts in atypical presentations, particularly when coexisting inflammatory dermatoses such as seborrheic dermatitis obscure the clinical picture.
References
1. Mahajan K, Relhan V, Relhan AK, Garg VK. Pityriasis rosea: an update on etiopathogenesis and management of difficult aspects. Indian J Dermatol. 2016;61(4):375-384. doi:10.4103/0019-5154.185699
2. Trayes KP, Savage K, Studdiford JS. Annular lesions: diagnosis and treatment. Am Fam Physician. 2018;98(5):283-291.
3. Mahroum N, Shoenfeld Y. Classic pityriasis rosea. Isr Med Assoc J. 2022;24(8):549.
4. Litchman G, Nair PA, Syed HA, et al. Pityriasis rosea. In: StatPearls [Internet]. StatPearls Publishing; 2024.
5. Leung AKC, Lam JM, Leong KF, Hon KL. Pityriasis rosea: an updated review. Curr Pediatr Rev. 2021;17(3):201-211. doi:10.2174/1573396316666200923161330
6. VanRavenstein K, Edlund BJ. Diagnosis and management of pityriasis rosea. Nurse Pract. 2017;42(1):8-11. doi:10.1097/01.NPR.0000511012.21714.66
7. Gandhi J, Agrawal S, Gupta S, Verma K, Mohite A. Pattern of papulosquamous disorders in children: a clinico-epidemiological study. Cureus. 2022;14(1):e21194. doi:10.7759/cureus.21194
8. Polat M, Yildirim Y, Makara A. Palmar herald patch in pityriasis rosea. Australas J Dermatol. 2012;53(3):e64-e65. doi:10.1111/j.1440-0960.2011.00808.x
9. Robati RM, Toossi P. Plantar herald patch in pityriasis rosea. Clin Exp Dermatol. 2009;34(2):269-270. doi: 10.1111/j.1365-2230.2008.02772.x
10. Ciccarese G, Drago F. Atypical presentations of pityriasis rosea: a reply. Dermatol Online J. 2017;23(8):13030/qt2d50q1tq. doi:10.5070/D3238036020
11. Fölster-Holst R, Zawar VP, Chuh A. Paraviral exanthems. Expert Rev Anti Infect Ther. 2016;14(6):601-611. doi:10.1080/14787210.2016.1184084
12. Makhecha M, Singh T, Khatib Y. Dermoscopy to differentiate guttate psoriasis from pityriasis rosea—a mimicker. Dermatol Pract Concept. 2021;11(1):e2021138. doi:10.5826/dpc.1101a138
13. Vasisht S, Kansal NK. Dermoscopic features of pityriasis rosea. BMJ Case Rep. 2023;16(10):e256304. doi:10.1136/bcr-2023-256304
14. Thomas M, Khopkar U. Salute sign: a nonambiguous histopathological sign in pityriasis rosea. Indian Dermatol Online J. 2016;7(6):543-544. doi:10.4103/2229-5178.193917
15. Leung AKC, Barankin B, Lam JM, Leong KF. Childhood guttate psoriasis: an updated review. Drugs Context. 2023;12:2023-8-2. doi:10.7573/dic.2023-8-2
16. Flamm A, Alcocer VM, Kazlouskaya V, Kwon EJ, Elston D. Histopathologic features distinguishing secondary syphilis from its mimickers. J Am Acad Dermatol. 2020;82(1):156-160. doi:10.1016/j.jaad.2019.07.011
17. Chaudhry S, Akinlusi I, Shi T, Cervantes J. Secondary syphilis: pathophysiology, clinical manifestations, and diagnostic testing. Venereology. 2023;2(2):65-75. doi:10.3390/ venereology2020006
18. Dall’Oglio F, Nasca MR, Gerbino C, Micali G. An overview of the diagnosis and management of seborrheic dermatitis. Clin Cosmet Investig Dermatol. 2022;15:1537-1548. doi:10.2147/CCID.S284671
19. Sawitri PD, Karmila IGAAD, Sadeli MS. Dermoscopy in superficial fungal infection. Bali Dermatol Venereol J. 2021;4(2):35-39. doi:10.15562/bdv.v4i2.52
20. Leung AKC, Lam JM, Leong KF, Hon KL. Tinea corporis: an updated review. Drugs Context. 2020;9:2020-5-6. doi:10.7573/dic.2020-5-6
21. Żychowska M, Kołcz K. Dermoscopy for the differentiation of subacute cutaneous lupus erythematosus from other erythematous desquamative dermatoses— psoriasis, nummular eczema, mycosis fungoides and pityriasis rosea. J Clin Med. 2024;13(2):577. doi:10.3390/jcm13020577
22. Robinson CA, Love LW, Saleh HM, et al. Nummular dermatitis. In: StatPearls [Internet]. StatPearls Publishing; 2024.
23. Khachemoune A, Blyumin ML. Pityriasis lichenoides: pathophysiology, classification, and treatment. Am J Clin Dermatol. 2007;8(1):29-36. doi:10.2165/00128071- 200708010-00004
24. Alba-Rojas E, Guerra-Garza AS, Ocampo-Candiani J. Diagnostic dermoscopy in pityriasis lichenoides chronica and pityriasis lichenoides et varioliformis acuta: a case series. Dermatol Pract Concept. 2025;15(2):5078. doi:10.5826/dpc.1502a5078
25. Durgin JS, Whittington CP, Harrell J, Mervak JE, Smith EH. Clinicopathologic features of pityriasis rosea-like drug eruption secondary to imatinib: a case report and review of the literature. J Cutan Pathol. 2024;51(11):860-865. doi:10.1111/cup.14692
26. Sheern C, Levell NJ, Craig PJ, et al. Mycosis fungoides: a review. Clin Exp Dermatol. 2025;50(12):2365-2375. doi:10.1093/ced/llaf341
27. Villalon-Gomez JM. Pityriasis rosea: diagnosis and treatment. Am Fam Physician. 2018; 97(1):38-44.
28. Chang HC, Sung CW, Lin MH. The efficacy of oral acyclovir during early course of pityriasis rosea: a systematic review and meta-analysis. J Dermatolog Treat. 2019;30(3):288-293. doi:10.1080/09546634.2018.1508820