What Caused This Recurrent Eruption on the Neck, Ears, and Shoulders?

Case Report
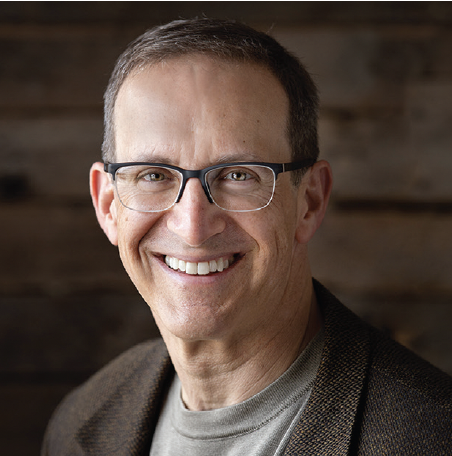
A 29-year-old woman presented for a dermatologic evaluation with erythematous pustular lesions involving the face, ear, neck, shoulder, and scapular areas (Figure 1). The lesions evolved in flares, with partial remissions over the past 4 to 5 years. The patient was previously treated inconsistently with corticosteroids and synthetic antimalarial drugs, yielding only partial improvement. Notably, she has had a history of chronic otitis media for the past 5 years.
What is your diagnosis?
Scroll below to find out!
Diagnosis: Acute Generalized Exanthematous Pustulosis
Acute generalized exanthematous pustolsis (AGEP) is a rare, severe cutaneous adverse reaction most commonly triggered by medications, particularly antibiotics; however, It can also be induced by other drugs, infections, or other exposures.1,2 In a large literature review of 297 patients, anti-infectives for systemic use were implicated in over one-third of events, particularly beta-lactam antibacterials and macrolides.3 Other notable drug classes include antineoplastics, anti-inflammatory or anti-rheumatic agents, and hydroxychloroquine, which alone was reported in nearly 13% of patients.3 Less frequent triggers encompass antivirals, vaccines, cardiovascular agents, and contrast media.3
Clinical Presentation
AGEP is characterized by the abrupt onset of dozens to hundreds of small, nonfollicular pustules on a background of edematous erythema, often accompanied by fever and leukocytosis, especially neutrophilia.2 The pustular eruption typically appears within 24 to 48 hours after contact with the causative agent and resolves within 2 weeks once the trigger is removed, followed by postpustular desquamation.1,4 Systemic involvement, such as hepatic, renal, or pulmonary dysfunction, occurs in a minority of cases and can be severe.5,6 Involvement of the mucous membranes is uncommon and, when present, is typically mild.7,8
Histology
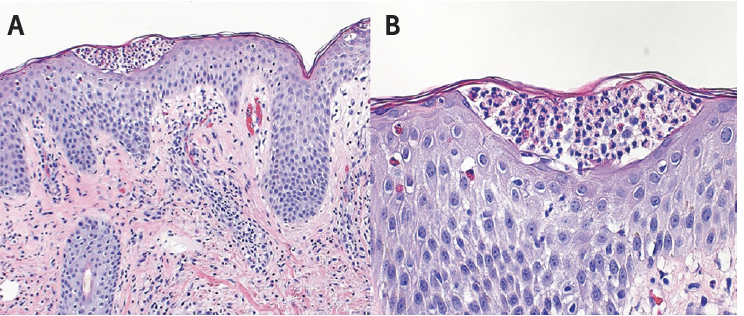
Histopathology of AGEP reveals subcorneal or intraepidermal pustules with papillary dermal edema and a mixed inflammatory infiltrate with neutrophils and eosinophils (Figure 2).1,6,8 Other diseases to consider in the histologic differential diagnosis include candidiasis, acropustulosis of infancy, transient neonatal pustular melanosis, generalized pustular psoriasis (GPP), impetigo, IgA pemphigus, subcorneal pustular dermatosis (SPD), staphylococcal scalded skin syndrome (SSSS), and erythema toxicum neonatorum.
Etiopathology
The pathogenesis of AGEP involves drug-specific T cells that release cytokines, especially IL-8, IL-17, and IL-36, resulting in neutrophil recruitment and pustule formation.2,5,9,10 Although the genetic basis is not yet fully clarified, mutations in IL-36RN appear to predispose certain individuals to the development of AGEP.2,9
Differential Diagnosis
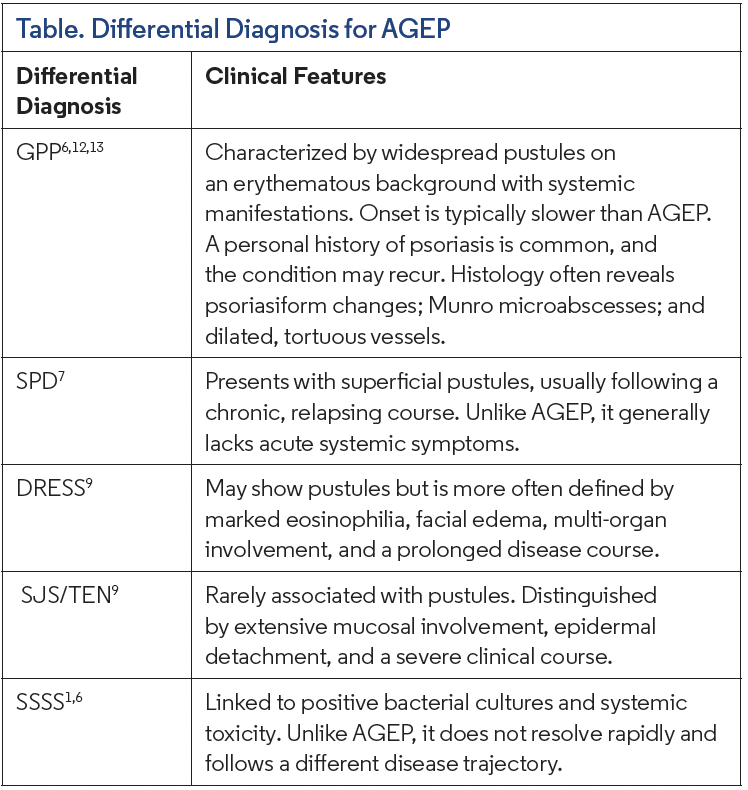
Differentiating AGEP can be difficult because its clinical presentation overlaps with several other disorders. The differential diagnosis includes GPP, SPD, drug reaction with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) and SSSS (Table).
The diagnosis of AGEP is based on clinical presentation and histopathology. To aid classification, the European Study of Severe Cutaneous Adverse Reactions group developed a 12-point scoring system that integrates morphology, clinical course, fever, laboratory results, and histologic findings.11 This system categorizes cases into 4 groups: no AGEP, possible AGEP, probable AGEP, and definitive AGEP.4,11
Management
Treatment centers on prompt discontinuation of the offending drug along with supportive care. While most cases resolve spontaneously, more severe or persistent presentations may necessitate systemic corticosteroids and, in rare situations, alternative immunosuppressive agents.
Our Patient
In this case, the diagnosis of AGEP was made based on the clinical distribution of numerous nonfollicular pustules on an erythematous base, the history of recurrent flares associated with medication exposure, and the temporal relationship to amoxicillin prescribed for otitis media. Following discontinuation of amoxicillin, the patient’s pustular eruption cleared, supporting the diagnosis of drug-induced AGEP. The patient was subsequently lost to follow up, and longer-term outcomes could not be assessed.
Conclusion
AGEP is typically self-limited once the causative agent is removed. Prognosis is favorable, although severe systemic involvement can occur in some cases. Early recognition and discontinuation of the offending drug are crucial for a positive outcome. Management often includes supportive care, and systemic corticosteroids may be necessary for more severe cases. While most patients recover without long-term complications, close monitoring is essential to identify any potential systemic involvement that could impact recovery. Long-term follow up is recommended to assess for recurrence or delayed complications, especially in cases with significant systemic symptoms.
References
1. Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015;73(5):843-848. doi:10.1016/j. jaad.2015.07.017
2. Feldmeyer L, Heidemeyer K, Yawalkar N. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Int J Mol Sci. 2016;17(8):1214. doi:10.3390/ijms17081214
3. Vallejo-Yagüe E, Martinez-De la Torre A, Mohamad OS, Sabu S, Burden AM. Drug triggers and clinic of acute generalized exanthematous pustulosis (AGEP): a literature case series of 297 patients. J Clin Med. 2022;11(2):397. doi:10.3390/ jcm11020397
4. Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP)—a clinical reaction pattern. J Cutan Pathol. 2001;28(3):113-119. doi:10.1034/j.1600-0560.2001.028003113.x
5. Stadler PC, Oschmann A, Kerl-French K, et al. Acute generalized exanthematous pustulosis: clinical characteristics, pathogenesis, and management. Dermatology. 2023;239(3):328-333. doi:10.1159/000529218
6. Parisi R, Shah H, Navarini AA, et al. Acute generalized exanthematous pustulosis: clinical features, differential diagnosis, and management. Am J Clin Dermatol. 2023;24(4):557-575. doi:10.1007/s40257-023-00779-3
7. Hammerbeck AA, Daniels NH, Callen JP. Ioversol-induced acute generalized exanthematous pustulosis: a case report. Arch Dermatol. 2009;145(6):683-687. doi:10.1001/archdermatol.2009.100
8. Creadore A, Desai S, Alloo A, et al. Clinical characteristics, disease course, and outcomes of patients with acute generalized exanthematous pustulosis in the US. JAMA Dermatol. 2022;158(2):176-183. doi:10.1001/jamadermatol.2021.5390
9. Hadavand MA, Kaffenberger B, Cartron AM, Trinidad JCL. Clinical presentation and management of atypical and recalcitrant acute generalized exanthematous pustulosis. J Am Acad Dermatol. 2022;87(3):632-639. doi:10.1016/j. jaad.2020.09.024
10. Schmid S, Kuechler PC, Britschgi M, et al. Acute generalized exanthematous pustulosis: role of cytotoxic T cells in pustule formation. Am J Pathol. 2002;161(6):2079-2086. doi:10.1016/S0002-9440(10)64486-0
11. Sidoroff A, Dunant A, Viboud C, et al. Risk factors for acute generalized exanthematous pustulosis (AGEP)—results of a multinational case-control study (EuroSCAR). Br J Dermatol. 2007;157(5):989-996. doi:10.1111/j.1365- 2133.2007.08156.x
12. Halevy S, Kardaun SH, Davidovici B, Wechsler J, EuroSCAR and RegiSCAR study group. The spectrum of histopathological features in acute generalized exanthematous pustulosis: a study of 102 cases. Br J Dermatol. 2010;163(6):1245-1252. doi:10.1111/j.1365-2133.2010.09967.x
13. Benezeder T, Bordag N, Woltsche J, et al. IL-36-driven pustulosis: transcriptomic signatures match between generalized pustular psoriasis (GPP) and acute generalized exanthematous pustulosis (AGEP). J Allergy Clin Immunol. 2025;155(6):1913-1927. doi:10.1016/j.jaci.2025.01.046