The Modern Cath Lab Playbook: Angio FFR, Low-Contrast PCI, CMD Workflows, and AI
A Panel Discussion at CRT 2026’s Nurses and Technologists Session
A Panel Discussion at CRT 2026’s Nurses and Technologists Session
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
At CRT 2026 in Washington, DC, moderator Brian C. Case, MD; moderator Dionne P. Ross, MSN, RN, NE-BC; Allen Jeremias, MD; Bruce Samuels, MD; and Arnold H. Seto, MD, MPA, participated in a panel discussion on “How Imaging and Physiology Transform the Flow in the Cath Lab” during the Nurses and Technologists session. Panelists focused on where angiography-derived physiology, intravascular imaging, and coronary function testing are improving decision-making, and integrating these tools without overwhelming teams.

Imaging + Physiology: Better Data, But Only If the Acquisition Is Good
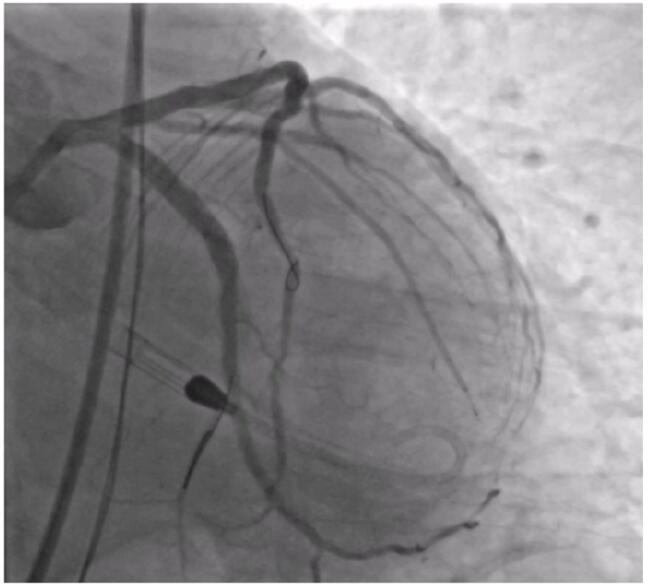
The panel began their discussion by considering where angio-derived fractional flow reserve (FFR) works and where it doesn’t. Dr. Seto noted it is not validated in left main or bifurcations, and angio FFR becomes less reliable when the angiogram is suboptimal, especially in highly tortuous segments. He added that when you have strong imaging, angio FFR can be very accurate.
Angio-derived FFR is not “one click and done,” the panelists noted. If the angiogram quality is poor, the physiology number can be off, so the team has to help capture clean, consistent views with as little overlap and foreshortening as possible, and enough angles for the system to build a reliable model.
Zero-Contrast and Low-Contrast PCI: Imaging Becomes the Steering Wheel
A major thread was the move toward zero-contrast or minimal-contrast percutaneous coronary intervention (PCI), particularly for patients with advanced renal dysfunction. When asked whether imaging is mandatory for true zero-contrast PCI, Dr. Jeremias answered, “Intravascular imaging is mandatory because that is how we steer the whole procedure. With newer OCT systems and rapid pullback, you could theoretically inject saline, so it is possible to do this with zero or close to zero contrast.”
He noted, however, that optical coherence tomography (OCT)-based zero-contrast workflows can become more complex because teams often rely on still frames to mark landing zones and translate imaging to the angiographic roadmap.
Dr. Jeremias described a shift away from “pure” zero-contrast PCI toward minimal-contrast strategies, using a single early roadmap image and a very small closing injection. “We have moved more towards minimal contrast rather than zero,” he said. “I think a 3 to 4 cc injection at the end, in the vast majority of cases, is well tolerated.”
Dr. Samuels reinforced that low-contrast technique should be practiced in routine cases and not be reserved only for patients with severe renal dysfunction. This can be accomplished by reducing extra angiographic views, avoiding frequent “puffing,” and leaning into intravascular ultrasound (IVUS) for confirmation rather than routine repeat contrast injections.
Dr. Seto raised the “final angiogram” question. He pointed out why teams often do it (to confirm the final result and look for wire perforation), then pressed on whether operators are comfortable skipping it and what the medico-legal risk might be. Dr. Seto brought up the example of a patient with a GFR of 8. The panel described contingency tactics: using IVUS to guide femoral access work, skipping the initial roadmap if prior angiography is available, and creating a “metallic silhouette” by wiring multiple branches to define anatomy without contrast before a minimal final check.
CMD: Why Normal Coronaries Are Not the End of the Story
The panel then moved to coronary microvascular dysfunction (CMD) and the implications for cath lab flow. Dr. Case explained why symptoms can persist despite normal-appearing epicardial vessels: angiography visualizes the “highways,” but the microvasculature regulates perfusion at the tissue level, and patients can have structural microvascular disease or endothelial-dependent spasm in large or small vessels.
He emphasized that normal angiography is common, and a substantial portion of those patients have microvascular disease contributing to symptoms.
Dr. Samuels noted that most of the coronary tree is beyond the resolution of routine cath imaging, and a large fraction of angina referrals ultimately have no severe obstruction to fix. Yet these patients are often dismissed in ways that worsen outcomes and trust. “Too often we tell these patients, ‘You’re fine, it’s not your heart,’ but we’re doing them a disservice,” Dr. Samuels said. “They have the lowest quality of life, and they are suffering. It is on us to diagnose whether they actually have medium- and small-vessel disease.”
The group positioned coronary function testing as an extension of physiologic assessment to not only explain symptoms, but to guide targeted therapy, and reduce repeat visits and repeat invasive evaluations.
What’s Next: Angiography-Based Microvascular Metrics
Looking to the future, the panel predicted rapid growth in non-wire, angiography-based microvascular assessment (angio CFR [coronary flow reserve] / angio IMR [index of microcirculatory resistance]). Dr. Samuels anticipated early-generation solutions that quantify flow via dye transit/timing, myocardial blush, and pixel-based motion analysis, which would extract information about microcirculatory resistance from how contrast moves through the bed.
The panel’s caution was that these angio-based physiology tools are only as good as the assumptions the software makes about the microcirculation. The biggest factor in accuracy is what the algorithm assumes is happening in the small vessels. Early versions will likely estimate from what is seen on angiography: how fast the dye moves, the extent of myocardial blush, and possibly pixel-based measurements, so if those signals are unclear, the number can be misleading.
Making Coronary Function Testing Workable: Ad Hoc vs Planned, and the Acetylcholine Bottleneck
For cath lab teams, one of the most practical points was the difference between ad hoc function testing right after diagnostic angiography versus planned testing. Dr. Case described both models, but noted that planned testing can have higher diagnostic yield because the team can instruct patients to hold medications (e.g., calcium channel blockers, beta blockers, nitrates) for a defined period pre-procedure and arrive prepared to run the full protocol.
Dr. Samuels identified the barrier that often determines whether labs can do ad hoc testing reliably: acetylcholine availability and workflow, since full testing typically includes both adenosine-mediated assessment and acetylcholine provocation for spasm.
He also challenged symptom-only triage: exertional angina is not a reliable discriminator between CMD and spasm, and even with thoughtful outpatient workups (including PET/MRI in some cases), many symptomatic patients ultimately seek a definitive diagnosis in the cath lab.
The Human and Operational Side: Buy-In and Competencies
A question from the audience focused on a core challenge: labs are layering angio-FFR, intravascular imaging, coronary function testing, and emerging non-wire physiology, often on top of existing integration gaps. Staff are being asked to learn and manage a lot of new technology at once, sometimes resulting in concern and skepticism that it may be “just adding time” to cases.
Panelists argued buy-in is built the same way as any complex lab capability: repeatable education, trained champions, and clear time/role allocation. Labs rely on multiple in-services and dedicated angio FFR champions; importantly, with enough redundancy to cover turnover and absences.
Dr. Case emphasized that when staff understand why a pressure wire is going down a normal artery, adoption accelerates, and the best signal of buy-in is when staff start asking why CMD testing isn’t being done.
Dr. Samuels said the patient response can be a powerful motivator for the team. After testing, when he tells a patient, “We figured out what your problem is, and we’re going to treat you,” he often sees an immediate reaction: “Tears start to come down. It is very impactful.”
Finally, the group discussed medication handling and competency maintenance around acetylcholine. Dr. Seto described keeping acetylcholine accessible (via Omnicell) with nurses mixing at the point of care, while acknowledging Joint Commission concerns and the need for competency and policy alignment.
Dionne P. Ross, MSN, RN, NE-BC, highlighted practical constraints like expiration dates and how pharmacy responsiveness can sometimes be the safest path. “We have to be careful because certain medications have expiration dates, so we don’t want to keep acetylcholine in our Pyxis or readily available,” she said. “Our pharmacy functions fairly quickly, so we request it as soon as we need it, or when we know an upcoming case will require it.”
Where the Workflow is Heading: CT-First Planning and AI Augmentation
To close, the panel discussed how CT planning is starting to move into the cath lab workflow, especially for stable angina/elective outpatient cases. Dr. Seto said that interventionalists such as Emmanouil Brilakis and others are working to encourage reviewing a CT before the case and using it to plan aspects such as which guides to use, appropriate access, and whether to be ready with atherectomy, so the team always has imaging reviewed beforehand as part of the timeout and has fewer surprises. Dr. Jeremias noted this type of procedural planning is harder to do for many inpatients and acute coronary syndrome cases, where there isn’t time to get a CT first.
The panel also discussed how AI is coming and will show up in both coronary angiography and intravascular imaging. “It is already being used routinely in radiology,” said Dr. Jeremias. “I expect we will see it in the cath lab as well.” AI will help the team by pointing to the location of the tightest stenosis, suggesting stent length, and producing more automated measurements. We are already seeing early versions of this ability in OCT and IVUS systems, said Dr. Jeremias, including automated readings and automated calcium detection, and he predicted that in the coming years, performing an angiogram will increasingly prompt a broad set of data to appear on the screen in real time.