Bioresorbable Scaffolds in BTK Disease: Where We Are and Where We’re Headed
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.

Auckland City Hospital, New Zealand
During a Tuesday afternoon session, ISET 2026 Career Achievement Award Recipient Andrew Holden, MBChB, FRANZCR, delivered a comprehensive and forward-looking overview of bioresorbable scaffold technology for below-the-knee (BTK) disease, with a particular focus on chronic limb-threatening ischemia (CLTI). Dr Holden framed bioresorbable drug-eluting scaffolds as a meaningful evolution in a therapeutic space that has long struggled to deliver durable outcomes.
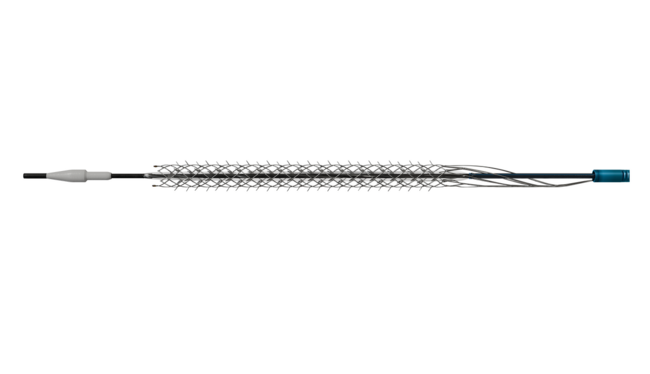
The presentation opened by acknowledging the limitations of current BTK treatment strategies and the historical lack of randomized data demonstrating superiority over plain balloon angioplasty. He then discussed the LIFE-BTK randomized controlled trial (RCT) evaluating the Esprit™ BTK everolimus-eluting resorbable scaffold (Abbott Cardiovascular). Dr Holden highlighted that LIFE-BTK is the first successful RCT to show clear superiority of an investigational device over standard percutaneous transluminal angioplasty in patients with CLTI. At 1 year, the Esprit BTK scaffold delivered a striking improvement in the composite endpoint of limb salvage and primary patency, with benefits that were consistent across lesion lengths and accompanied by favorable safety outcomes.
For clinicians thinking beyond short-term patency curves, the data did not stop at 12 months. Dr Holden walked through 2- and 3-year follow-up results demonstrating sustained clinical advantage, lower restenosis rates, reduced need for clinically driven target lesion revascularization, and ongoing improvement in Rutherford-Becker classification. These longer-term findings reinforced the idea that bioresorbable scaffolds may positively influence disease progression rather than simply delaying restenosis.
The session also explored emerging and complementary technologies shaping the future of BTK intervention. Early and mid-stage data from additional platforms, including the MAGNITUDE® scaffold (R3 Vascular) studied in the RESOLV I and ELITE-BTK IDE trials and the MOTIV® bioresorbable scaffold platform (REVA Medical), suggested a growing body of evidence supporting consistent patency, low reintervention rates, and meaningful wound-healing outcomes. Together, these studies point toward a broader class effect rather than a single-device phenomenon.
Dr Holden closed by addressing the practical and unanswered questions that remain most relevant to everyday practice. These included how bioresorbable scaffolds perform in longer and more complex lesions, when they should be used as a primary strategy vs a bailout option, how they compare with balloon-expandable drug-eluting stents, and how cost-effectiveness data will translate across healthcare systems and geographies. Bioresorbable scaffolds are no longer a future concept in BTK disease, Dr Holden said, but an increasingly data-backed option that may redefine standards of care for patients with CLTI.