


How Rethinking Classification of Psoriasis Severity Can Help Patients Find Their Effective Therapies Sooner
Psoriasis management has evolved rapidly over the past decade. The availability of advanced treatments with established efficacy and well-characterized safety profiles has redefined treatment possibilities for patients. Despite these advances, many dermatologists rely on outdated frameworks for characterizing disease severity that no longer support optimal use of current treatment options or the lived experiences of psoriasis patients.
Traditional guidelines and payer criteria have struggled to keep pace with the evolution of advanced therapies for psoriasis. As a result, some patients who might potentially benefit from systemic therapy remain undertreated. Recognizing this disconnect, the International Psoriasis Council (IPC) recently published two communications designed to provide practical, evidence-based guidance that clinicians can implement for real-world impact.1,2
Together, these communications - one reclassifying psoriasis disease severity, and the other, a consensus statement on defining topical therapy failure - form a clear call to action for the dermatology community: reassess how psoriasis severity is defined and intervene earlier when topical therapy is insufficient to broaden eligibility for advanced treatment.
Why the IPC Revisited Psoriasis Severity Classification Now
For decades, psoriasis has been broadly categorized as mild, moderate, or severe, with severity often anchored to objective measures such as body surface area (BSA) involvement and the Psoriasis Area and Severity Index (PASI). In clinical trials and many reimbursement frameworks, BSA ≥10% or PASI score ≥12 has traditionally defined moderate-to-severe disease.
While these metrics remain valuable in research settings, their limitations in everyday clinical practice are well recognized. PASI is complex and not calculated routinely, and neither PASI nor BSA adequately captures how psoriasis affects patients’ daily functioning, self-image, and emotional well-being, especially when lesions involve visible or sensitive “high impact” areas.
In real-world practice, many patients experience a substantial disease burden despite limited BSA involvement. Psoriasis affecting the face, scalp, palms, soles of the feet, or genital region can interfere with work, social interactions, intimacy, and basic activities of daily living. Over time, this persistent burden can contribute to anxiety, depression, and cumulative quality-of-life impairment, even when the disease might be classified as “mild” using traditional criteria.
“Severity in clinical practice must reflect not only what we see on the skin, but the cumulative impact psoriasis has over time,” said Peter van de Kerkhof, MD, PhD, Emeritus Professor of dermatology at the Radboud University Nijmegen Medical Centre and current IPC chief medical officer. “When disease is inadequately controlled, it can affect self-confidence, social development, and quality of life for years. There is also growing recognition that psoriasis is a systemic inflammatory condition that may progress and be associated with comorbidities such as psoriatic arthritis, inflammatory bowel disease, and cardiovascular risk. This is why earlier, more effective intervention represents a window of opportunity to alter the entire disease course, not just manage the skin manifestations.”
The IPC revisited severity classification to address the misalignment of clinician-determined numeric thresholds and lived patient experience. By evolving the psoriasis severity framework, the IPC is ensuring that patients experiencing meaningful impact of their disease are not excluded from appropriate systemic therapy solely because they fail to meet rigid cutoffs.
The Revised IPC Disease Severity Framework: What’s New
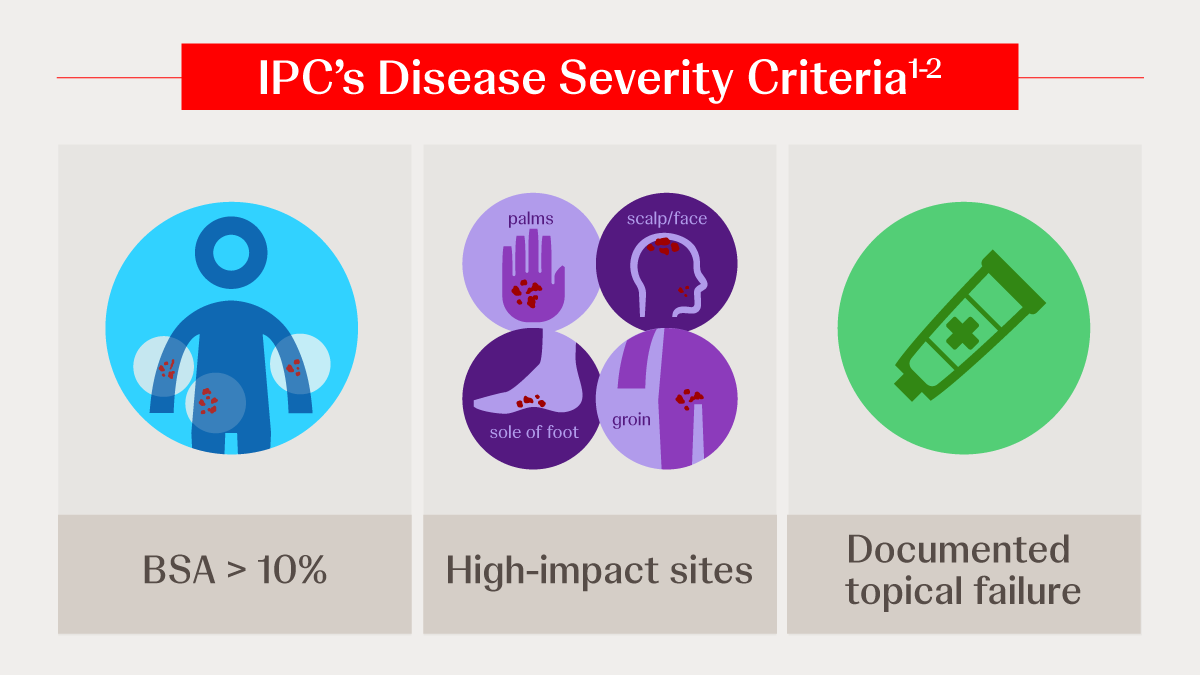
The IPC’s updated framework defines psoriasis severity using three pragmatic criteria:
- BSA >10%
- Involvement of high-impact body sites, including the face, scalp, palms, soles of the feet, and groin
- Documented failure of topical therapy
Meeting any one of these criteria may warrant consideration of systemic therapy.
This represents an important conceptual shift. This framework no longer defines psoriasis severity exclusively by the extent of skin involvement, but also by broader parameters including functional limitation, disease impact, and inadequate response to topical therapy. High-impact sites were specifically included because evidence consistently shows that involvement of these areas disproportionately affects quality of life and treatment satisfaction, regardless of overall BSA.
“This framework aligns with real-world clinical observations and decision-making,” Dr. van de Kerkhof said. “It acknowledges that visible or functionally limiting disease - even with modest surface area involvement - can justify a more proactive treatment approach.”
Importantly, the IPC framework is gaining global traction, with early adoption reflected in country-specific guideline discussions and consensus documents.1 For practicing dermatologists, it offers a simpler, more inclusive method for identifying patients who may benefit from systemic therapy while remaining grounded in expert consensus.
Topical Treatment Failure: Clarifying a Long-Standing Gray Area
Topical therapies remain foundational in psoriasis management; however, ambiguity regarding topical treatment failure has historically led to prolonged use of therapies that may provide limited benefit, delaying transition to potentially effective options.
The recent IPC communication published in the Journal of the American Academy of Dermatology (JAAD), addresses a long-standing need for clarity by defining topical failure in practical terms. Failure may be considered when an appropriate topical regimen, generally consisting of two treatment cycles of approximately four weeks each, fails to achieve meaningful improvement. Topical therapy may also be deemed unsuccessful when it cannot be used adequately due to sensitivity in high-impact areas, adherence challenges, or persistent quality-of-life impairment.
This definition emphasizes timely reassessment rather than continuing ineffective treatment and recognizes that prolonged incremental adjustments to topical therapy can contribute to patient frustration, poor adherence, and ongoing disease burden - often without meaningful clinical gains.
“In clinical practice, when an appropriate topical regimen does not lead to substantial improvement within a reasonable timeframe, it is unlikely to deliver adequate long-term control,” Dr. van de Kerkhof explained. “At that point, escalation to another therapeutic approach should be thoughtfully considered.”
The IPC communication now explicitly defines topical failure, one of the three criteria for characterizing psoriasis based on the new IPC disease severity assessment framework, providing clinicians with structured, evidence-based triggers for reevaluating treatment strategy.
Why Rethinking Eligibility for Systemic Therapy Matters
Despite the availability of effective advanced therapies, several barriers continue to delay transitioning patients to such treatments. Some dermatologists remain cautious due to lingering concerns that biologics are broadly immunosuppressive, despite extensive safety data supporting IL-17 and IL-23 inhibition.3 Others face administrative challenges, including documentation requirements and payer criteria that may not yet reflect the updated psoriasis severity definition.
There is also a longstanding treatment mindset to escalate therapy only after prolonged periods of partial control, particularly when patients suggest that their outcomes are “good enough.” However, this approach may overlook the cumulative physical and psychosocial burden of ongoing inflammation, especially in patients with high-impact site involvement.
“There has been a tendency in some practices to defer systemic treatment until patients meet rigid numerical thresholds,” said Bruce Strober, MD, PhD, Clinical Professor of dermatology at Yale University School of Medicine. “The goal of the IPC’s rapid communications is to provide succinct, evidence-based guidance that reflects both modern therapies and contemporary clinical priorities.”
Rapid Communications as a New Clinical Currency
A defining feature of the IPC’s consensus approach is its publishing of rapid communications in the dermatology literature. Rather than relying solely on comprehensive guideline updates that may take months or years to complete, the IPC has adopted issuing focused statements to address pertinent clinical questions and improve timely decision-making.
This approach reflects an intentional effort to keep pace with emerging data and real-world clinical needs. These communications complement traditional guidelines and represent a model that may extend to other dermatologic diseases in the future.
Practical Takeaways for Dermatologists
- Assess severity using the IPC’s framework of three criteria, not BSA ≥10 alone.
- Account for the disproportionate impact of high-impact sites on patients’ quality of life, even with limited surface area involvement.
- Identify topical failure as defined by the IPC to avoid unnecessary delays in escalation of treatment.
- Understand the safety profiles of advanced therapies considering contemporary evidence.
- Integrate IPC rapid communications as authoritative, evidence- and consensus-based guidance when navigating evolving practice questions.
References
- Strober BE, Blauvelt A, van de Kerkhof PC, et al. International Psoriasis Council psoriasis disease severity reclassification: Update on validity, acceptance, and implementation. J Am Acad Dermatol. 2025;93(4):1154-1157. doi:10.1016/j.jaad.2025.05.1445
- Strober BE, Blauvelt A, van de Kerkhof PCM, et al. Establishing consensus on defining failure of topical therapy in psoriasis: Recommendations from the International Psoriasis Council. J Am Acad Dermatol. Published online September 11, 2025. doi:10.1016/j.jaad.2025.08.116
- Lebwohl, M.G., Carvalho, A., Asahina, A. et al. Biologics for the Treatment of Moderate-to-Severe Plaque Psoriasis: A Systematic Review and Network Meta-analysis. Dermatol Ther (Heidelb) 15, 1633–1656 (2025). https://doi.org/10.1007/s13555-025-01423-0













