What Caused This Truncal Rash?

Case Report
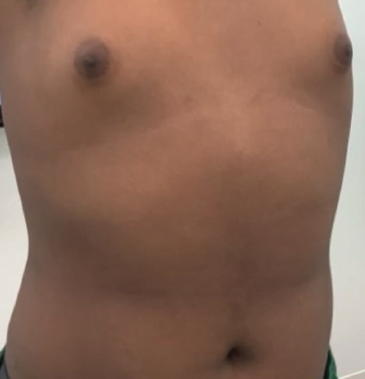
A 16-year-old African American adolescent boy with no known past medical history presented with a dark eruption involving the chest and abdomen ongoing for 1 year. He denied pruritus or other associated symptoms. His only medication was guanfacine for attention-deficit/hyperactivity disorder. The patient was previously treated for suspected tinea versicolor with ketoconazole shampoo and cream, but no improvement was seen. Physical examination revealed hyperpigmented patches with minimal overlying scale in a confluent pattern on the lateral chest and lateral abdomen, both wrapping ventromedially (Figure 1).
What is your diagnosis?
Scroll below to find out!
Diagnosis:
Confluent and Reticulated Papillomatosis
Confluent and reticulated papillomatosis (CARP) was first described and named by Gougerot and Carteaud in 1927 and 1928.1 Classic pathophysiology presents as an eruption of hyperkeratotic and hyperpigmented scaly plaques in the sternal region and midline of the back. The plaques tend to arrange in a confluent pattern in the sternal region and a reticulated pattern more peripherally.1 Although the trunk has majority involvement, the neck and axillae are often affected as well.2
Epidemiology and Etiology
CARP is an acquired dermatosis of unknown etiology that affects young adolescents to young adults, primarily ages 8 to 32 years, with males showing a higher incidence than females at a ratio of 1.4 to 2.6:1.3
There are several theories for the cause of CARP, including disordered keratinization in the epidermis. CARP has been posited as a variant of acanthosis nigricans, given that these entities appear similar on histopathology, with papillomatosis and hyperkeratosis with slight basilar pigmentation and an absence of dermal inflammatory infiltrate. Increased insulin levels activate epidermal proliferation factors, such as insulin-like growth factor 1, the tyrosine kinase receptor superfamily, epidermal growth factor, and fibroblast growth factor, and these enzymes may affect skin changes consistent with both CARP and acanthosis nigricans. Some cases of CARP have improved with weight loss and glucose control;3,4 however, a direct causal association between type 2 diabetes mellitus and CARP has not been firmly established.
Other theories have suggested that CARP’s primary etiology arises from infectious causes. Malassezia furfur has been suggested as a trigger due to the clinical similarities between CARP and tinea versicolor and its partial response to antifungal treatments. More recent studies also point to the Dietzia papillomatosis bacterium, a gram-positive aerobic actinomycete that has been isolated from patients diagnosed clinically with CARP.4,5 The bacterial theory appears plausible given that the most effective CARP treatments typically involve tetracycline antibiotics.
Histopathology
Although CARP is largely a clinical diagnosis, histopathologic findings can be helpful in differentiating from other similar conditions. Histologic findings typically show hyperkeratosis with epidermal papillomatosis, mild acanthosis, hypermelanosis of the basal layer, and a decreased granular layer. Under electron microscopy, an increased number of lamellar granules, increased transitional cells between the stratum granulosum and stratum corneum, and increased melanosomes in the stratum corneum may also be seen.4,6,7
Clinical Differential Diagnosis
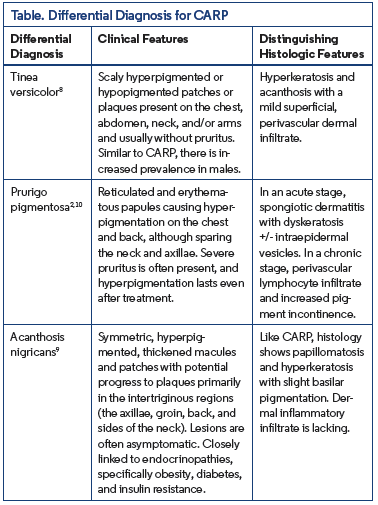
In addition to CARP, the differential diagnosis for a patchy eruption on the trunk with peripheral reticulation and central confluence includes tinea versicolor, prurigo pigmentosa, and acanthosis nigricans2,8-10 (Table).
Treatment
The most effective treatment for CARP thus far has proven to be oral minocycline 50 to 100 mg twice daily for 6 to 12 weeks. Studies have also shown that oral macrolides provide a good second alternative, specifically azithromycin 250 to 500 mg 3 times weekly for 3 weeks. It is believed that these medications have shown strong resolve due to their antibacterial and anti-inflammatory properties.4,11 Oral retinoids, such as isotretinoin, acitretin, and etretinate, have proven useful as an alternative oral treatment, although they are not recommended due to the efficacy of minocycline and azithromycin. Topical therapies, such as topical retinoids, urea, calcipotriol, and tacrolimus, have also proven successful.3,4 Recurrence has been seen after stopping treatment; an extended therapy regime and/or alternative therapy usage may be required.12
Our Patient
The patient was placed on 100 mg minocycline twice daily for 8 weeks, at which point the CARP had resolved (Figure 2).
Conclusion
CARP is characterized by a hyperpigmented eruption in the chest and abdomen, often extending to the axillae and neck. Its cause is unknown and it is typically asymptomatic. Due to its pattern and presentation, CARP can be misdiagnosed as tinea versicolor or prurigo pigmentosa and may sometimes be considered a variant of acanthosis nigricans. Diagnosis is largely clinical. First-line treatment of CARP consists of oral minocycline twice daily for 6 to 12 weeks. Topical or oral retinoids and antifungals may also serve as adjunctive therapies, although a wide variety of treatments have also shown efficacy.
References
1. El-Tonsy MH, El-Benhawi MO, Mehregan AH. Confluent and reticulated papillomatosis. J Am Acad Dermatol. 1987;16(4):893-894. doi:10.1016/s0190- 9622(87)80242-6
2. Shevchenko A, Valdes-Rodriguez R, Hsu S, Motaparthi K. Prurigo pigmentosa: case series and differentiation from confluent and reticulated papillomatosis. JAAD Case Rep. 2017;4(1):77-80. doi:10.1016/j.jdcr.2017.07.027
3. Lim JHL, Tey HL, Chong WS. Confluent and reticulated papillomatosis: diagnostic and treatment challenges. Clin Cosmet Investig Dermatol. 2016;9:217-223. doi:10.2147/CCID.S92051
4. Le C, Bedocs PM. Confluent and reticulated papillomatosis. In: StatPearls [Internet]. StatPearls Publishing; 2025.
5. Jones AL, Koerner RJ, Natarajan S, Perry JD, Goodfellow M. Dietzia papillomatosis sp. nov., a novel actinomycete isolated from the skin of an immunocompetent patient with confluent and reticulated papillomatosis. Int J Syst Evol Microbiol. 2008;58(Pt 1):68-72. doi:10.1099/ijs.0.65178-0
6. Jimbow M, Talpash O, Jimbow K. Confluent and reticulated papillomatosis: clinical, light and electron microscopic studies. Int J Dermatol. 1992;31(7):480-483. doi:10.1111/j.1365-4362.1992.tb02694.x
7. Lee SH, Choi EH, Lee WS, Kang WH, Bang DS. Confluent and reticulated papillomatosis: a clinical, histopathological, and electron microscopic study. J Dermatol. 1991;18(12):725-730. doi:10.1111/j.1346-8138.1991.tb03164.x
8. Karray M, McKinney WP. Tinea versicolor. In: StatPearls [Internet]. StatPearls Publishing; 2025.
9. Hughes EK, Brady MF, Rawla P. Acanthosis nigricans. In: StatPearls [Internet]. StatPearls Publishing; 2025.
10. Shaker N, Sathe NC. Prurigo pigmentosa. In: StatPearls [Internet]. StatPearls Publishing; 2025.
11. Scheinfeld N. Confluent and reticulated papillomatosis: a review of the literature. Am J Clin Dermatol. 2006;7(5):305-313. doi:10.2165/00128071-200607050-00004
12. Davis MDP, Weenig RH, Camilleri MJ. Confluent and reticulate papillomatosis (Gougerot–Carteaud syndrome): a minocycline-responsive dermatosis without evidence for yeast in pathogenesis. A study of 39 patients and a proposal of diagnostic criteria. Br J Dermatol. 2006;154(2):287-293. doi:10.1111/j.1365- 2133.2005.06955.x