

Electrical Cardioversion for Atrial Fibrillation in the Modern Era
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(3).
Bradley P Knight, MD, FACC, FHRS
Dear Readers,
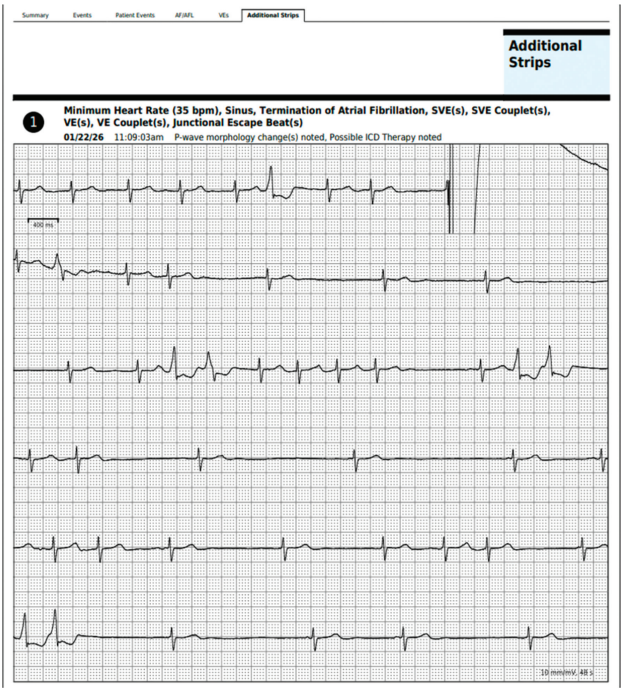
The rhythm strip below (Figure) was encountered during physician over-reading of a wearable 2-week patch monitor. What can be seen and what occurred?
The rhythm strip shows atrial fibrillation (AF). At the end of the first line, there is large spike signal superimposed on the QRS that briefly saturates the recording before the baseline is restored. The spike is followed by termination of the AF followed by sinus bradycardia interspersed with self-terminating episodes of atrial and ventricular arrhythmias. The preliminary interpretation by the technician proposes that an explanation for the conversion to sinus rhythm was a shock from an implantable cardioverter-defibrillator (ICD). This explanation for the large signal, however, is unlikely. Inappropriate therapy by an ICD for AF occurs when the ventricular rate is rapid and exceeds the cutoff rate of the defibrillator. In this case, the ventricular rate during AF is not fast. A review of the medical records confirmed that this patient actually underwent an elective external electrical cardioversion at the time of the recording. It was surprising (but not unreasonable) that the patch monitor was left on the patient at the time of the procedure. Nonetheless, this fortuitously recorded tracing highlights several issues associated with electrical cardioversion. It demonstrates that most patients do not convert cleanly to sinus rhythm and instead experience transient bradycardias and tachycardias following conversion. It also raises questions about the outcomes of electrical cardioversion in the modern era.
Early studies of electrical cardioversion for AF identified predictors of recurrence, such as the duration of the AF and left atrial enlargement. Subsequent studies focused on strategies to improve acute success rates, including studies in the early 1990s when biphasic waveforms were incorporated into external defibrillators.1 Techniques were developed to reduce the likelihood of immediate recurrence of AF and to lower energy requirements, including the administration of intravenous ibutilide.2 Interestingly, despite improved cardiovascular medical therapy, the surge in catheter ablation procedures for AF, improved access to elective outpatient cardioversions, and anesthesia support for cardioversions, there is little in the literature related to the outcomes of electrical cardioversion in the modern era.
In a rare occurrence, a group in Spain published their modern outcomes associated with elective cardioversion for AF last year.3 Their center performed cardioversion in 243 patients. The average age was 68 years and 67% were male. The median CHADsVASC score was 3. Electrical cardioversion was initially successful in 93% of patients. All but 6 patients remained in sinus rhythm immediately after the cardioversion before they were discharged home. At 6 months, 49% of patients were in sinus rhythm, and at one year, 40% of patients were in sinus rhythm. These long-term success rates are similarly low to those from decades ago, supporting more aggressive treatments such as catheter ablation. Amiodarone use was a predictor of maintaining sinus rhythm; however, surprisingly, other factors—including delay to cardioversion, left atrial size, and other clinical factors—did not predict recurrence.
What was striking was that the wait times between the decision to cardiovert the patient and the actual cardioversion was 265 days. This may be specific to the health care system in that country, but it is incredibly long. Two-thirds of the patients were initially managed with rate control, and those patients had an even longer average wait time of 308 days. Although this modern study of electrical cardioversion for AF failed to show an increase in AF recurrence among patients who waited longer for the procedure, the average wait time was so long in these patients that it is likely that few patients underwent cardioversion soon enough to defeat the remodeling that occurs during AF and make a difference. There are sufficient data that the early rhythm control approaches in AF results in better outcomes.4
This Spanish study of cardioversion for AF highlights the need for more rapid referral access to electrical cardioversion in all health care systems. Cardioversion is not a procedure that should be delayed. There needs to be increased awareness among primary care doctors and general cardiologists that patients with persistent symptomatic AF are sometimes better served by promptly scheduling a cardioversion while waiting for an appointment with an electrophysiologist. Allowing any health care provider to order a cardioversion, having a dedicated semi-autonomous, nurse-driven cardioversion program, and combining a cardioversion with a transesophageal echocardiogram (TEE) into one procedure for patients who need a TEE prior to cardioversion can improve access.5
Disclosures: Dr Knight has served as a paid consultant to Medtronic and was an investigator in the PULSED AF trial. He has served as a consultant, speaker, investigator, and/or has received EP fellowship grant support from Abbott, AltaThera, AtriCure, Baylis Medical, Biosense Webster, Biotronik, Boston Scientific, CVRx, Philips, and Sanofi; he has no equity or ownership in any of these companies. Dr Knight reports payment or honoraria from Convatec for a lecture.
References
1. Mittal S, Ayati S, Stein KM, et al, for the ZOLL Investigators. Comparison of a novel rectilinear biphasic waveform with a damped sine wave monophasic waveform for transthoracic ventricular defibrillation. J Am Coll Cardiol. 1999;34(5):1595-1601. doi:10.1016/S0735-1097(99)00363-0
2. Oral H, Souza JJ, Michaud GF, et al. Facilitating transthoracic cardioversion of atrial fibrillation with ibutilide pretreatment. N Engl J Med. 1999;340(24):1849-1854. doi:10.1056/NEJM199906173402401
3. Abdullah A, Ramewal GS, Wright C, et al. Outcomes of patients undergoing elective DC cardioversion for atrial fibrillation: a district general hospital experience. J Healthc Qual Res. 2025 Sep 27:101167. doi:10.1016/j.jhqr.2025.101167
4. Kirchof P, Camm AJ, Goette A, et al., on behalf of the EAST-AFNET 4 Trial Investigators. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med. 2020;383(14):1305-1316. doi:10.1056/NEJMoa2019422
5. Strzelczyk TA, Kaplan RM, Medler M, Knight BP. Outcomes associated with electrical cardioversion for atrial fibrillation when performed autonomously by an advanced practice provider. JACC Clin Electrophysiol. 2017;3(12):1447-1452. doi:10.1016/j.jacep.2017.04.004

