

Improving Atrial Fibrillation Ablation Outcomes Through Integrated Mapping, Signal Clarity, and Workflow Efficiency
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(6):12-13.
Interview by Jodie Elrod
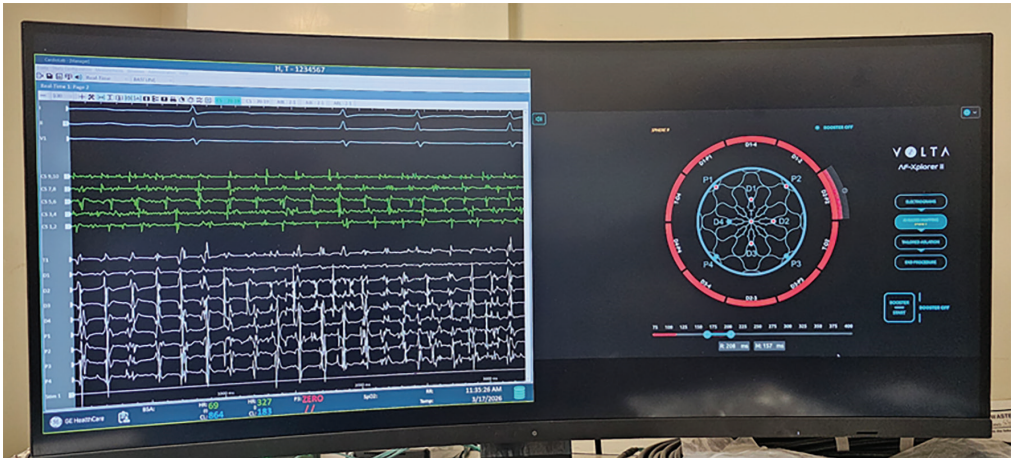
The first case of the EP Cath Command Center (GE HealthCare) and AF-Xplorer II (Volta Medical) in the United States was successfully completed by Paul Zei, MD, at Brigham and Women’s Hospital in Boston, Massachusetts. This interview explores initial impressions, signal fidelity and clarity, workflow connectivity, and the potential future impact of this technology in electrophysiology.
As the first physician in the United States to use this interface with the EP Cath Command Center and AF-Xplorer II, what were your initial impressions during the first case?
 One word, positive. The main challenges we face in the EP lab arise during cases where signal quality remains critically important—which is still true for much of EP work. We often struggle to maintain high-quality signals due to environmental noise in the lab. Performance also depends on the recording system and how the information is displayed through the user interface. That said, it is clear that a lot of thought went into making the system ergonomic and user-friendly. Overall, the experience was very positive.
One word, positive. The main challenges we face in the EP lab arise during cases where signal quality remains critically important—which is still true for much of EP work. We often struggle to maintain high-quality signals due to environmental noise in the lab. Performance also depends on the recording system and how the information is displayed through the user interface. That said, it is clear that a lot of thought went into making the system ergonomic and user-friendly. Overall, the experience was very positive.
How did the system perform in terms of signal fidelity?
Again, one of the biggest challenges is ambient noise in the room. We have an older lab, and because of years of added equipment, crossing wires, and modifications, it has become quite noisy in terms of electronic interference. While it will take more time to assess with full certainty, the signal quality so far appears very good.
Given the noise issue, there is much greater flexibility and variability in how filtering can be applied. This is important, because overfiltering can remove valuable signal content, while underfiltering can make the data difficult to interpret—so there is a “sweet spot.” The default settings seem to perform well in our lab environment. For us, this represents a notable improvement over what we had.
Can you describe the quality of and clarity of the streamed intracardiac signals, and how that may have influenced your clinical decision-making?
One important point to keep in mind from our run-through—both in evaluating the system and using it—is that, because of our setup, it was run in parallel with our current system. We didn’t shut off our existing recording system; instead, the signals were fed from it. This type of setup can sometimes lead to signal quality loss, but in this case, the signal quality was better than our existing system. We were able to do a side-by-side comparison, and there was a notable improvement, particularly in the intracardiac signals.

In terms of how this might influence decision-making—absolutely, it can. For those familiar with the Volta mapping system, you could almost avoid looking directly at the signals and rely solely on what AF-Xplorer identifies as a hotspot to guide ablation decisions. However, my perspective is that even with advanced mapping tools—like the modules available in other systems—it’s important to maintain a reality check by reviewing the raw electrograms.
By closely examining the signals and recognizing the patterns that define dispersion sites, you begin to see that these sites have characteristic signal qualities. Many of these—especially rapid, complex signals—require high fidelity, and there is a clear improvement in the fidelity of the signals we’re now seeing.
More than anything, this enhanced signal quality helps confirm whether a site truly demonstrates dispersion. As a result, the site belongs on the shortlist of targets for ablation.

How did the interface between the EP Cath Command Center and AF-Xplorer II impact your overall procedural workflow?
Because we were running it in parallel during our cases, I wasn’t relying solely on the new interface as my workflow, but I made a clear effort to focus most of my attention on it. One advantage is the interface of the Volta signals, which are displayed side by side with the raw Prucka signals.
As with most things in EP today, there are many different data inputs to monitor during a case—you’re layering in the map, intracardiac echocardiography, and the patient’s vitals. You must keep track of all of these simultaneously, and having the Volta data and raw Prucka data co-localized makes that process easier.
Do you see this type of interface solution enabling more efficient procedures compared to the traditional setup?
The ergonomics—specifically, how much effort it takes to view and process multiple data inputs—have led to incremental improvements in our procedural efficiency, since you don’t have to look in multiple places and things can move along more quickly. Just as importantly, for a center that uses Volta extensively, having the system readily configured and available saves a fair amount of time during procedure setup. While we haven’t formally measured this yet, I expect it will also improve room turnover time, as everything is essentially plug-and-play.
Were there any noticeable improvements you found advantageous?
This system definitely simplifies setup and streamlines the mapping process with Volta, particularly because of the side-by-side display. Additionally, while it’s a somewhat softer endpoint, the improved signal quality likely reduces the time needed to evaluate signals—if you choose to do so—because they are that much clearer.
What differentiates this solution from other technologies you’ve used, particularly in terms of interface, usability, and performance?
There’s nothing else quite like it—AF-Xplorer II’s interface within the GE HealthCare recording systems. In other setups, you’re typically placing an additional display in the corner of a multi-panel screen or adding a small secondary screen, which is a different experience. It also reflects GE HealthCare’s commitment to the value of the data Volta has presented. That data will likely continue to grow as an important tool in treating complex atrial fibrillation (AF) patients—particularly those who are redo cases or have persistent or longstanding persistent AF.
Based on your experience, where do you see this technology having the greatest impact in electrophysiology over the next few years?
We’re gradually evolving to a point where AF ablation, in particular, is splitting into 2 main types of procedures. We haven’t even touched on non-AF ablation—such as ventricular tachycardia ablation—where this kind of system could also be highly beneficial beyond the Volta context. For AF ablation, one category includes simpler, typically first-time anatomic procedures. With pulsed field ablation (PFA), these are often pulmonary vein isolation (PVI) or PVI-plus cases that can be completed in under an hour. The other category involves more complex cases—redos, longstanding persistent AF, or particularly challenging persistent AF—where we know more extensive intervention is required. In these cases, tools like Volta become important, especially given data showing significant improvement in outcomes, including greater freedom from AF. Traditionally, procedures using radiofrequency (RF) are noticeably longer. While PFA is now shortening that significantly, the complexity of these cases still demands more effort. Anything that improves workflow efficiency—such as a system with a strong digital connection like this—can make a meaningful difference. And it’s not limited to Volta; any approach that relies heavily on interpreting electrograms, as electrophysiologists should be doing, stands to benefit from this kind of data exchange paradigm.
The transcripts have been edited for clarity and length.
Disclosures: Dr Zei has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports support from GE HealthCare for consulting and lecture honoraria. He also reports support from Volta Medical for participation on a scientific advisory board, consulting, and research support.
This content was published with support from GE HealthCare.

