

CHAMPION-AF and the Future of Stroke Protection: Rethinking Left Atrial Appendage Closure and Patient Selection in Atrial Fibrillation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(6):16-19.
Interview by Jodie Elrod
In this interview with Christopher R. Ellis, MD, FACC, FHRS, we explore how CHAMPION-AF—alongside studies like CLOSURE-AF, OPTION, and OCEAN—might influence patient selection, clinical decision-making, and the future role of devices like WATCHMAN™ (Boston Scientific) in everyday practice. Dr. Ellis is the Director of the Atrial Fibrillation Center and LAA program at Vanderbilt Heart and Vascular Institute in Nashville, Tennessee.
What do the CHAMPION-AF trial results represent in the evolution of left atrial appendage closure (LAAC), and why is it an important moment for the field?
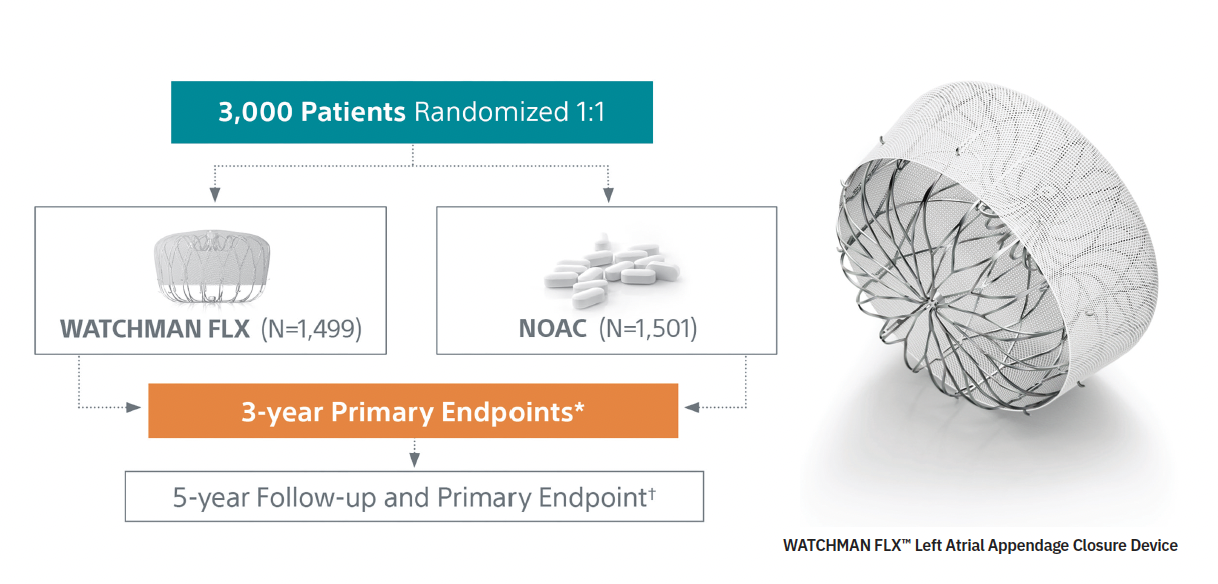
 CHAMPION-AF is the largest randomized trial to date comparing appendage closure versus anticoagulation. However, it was conducted using a prior-generation WATCHMAN FLX device—similar to the current WATCHMAN FLX™ PRO, but no longer available.
CHAMPION-AF is the largest randomized trial to date comparing appendage closure versus anticoagulation. However, it was conducted using a prior-generation WATCHMAN FLX device—similar to the current WATCHMAN FLX™ PRO, but no longer available.
Importantly, when the trial began, patients who were tolerating anticoagulation would not typically have been considered candidates for left atrial appendage occlusion (LAAO). Since enrollment, and leading up to the data presentation at the American College of Cardiology, several additional studies have emerged addressing similar patient populations.
As a result, while CHAMPION-AF marks a major milestone as the largest head-to-head drug-versus-device trial, its findings must be interpreted in the context of a now much broader and evolving body of evidence.
Can you comment on the primary endpoint outcomes and the net clinical benefit endpoint? How do you consider those when weighing options for patients?
In AF management, we balance symptom control, stroke protection, and bleeding risk. In CHAMPION-AF, the primary endpoint—a composite of cardiovascular death, systemic embolism, and stroke—addressed the core question of stroke protection: device versus anticoagulation.
The trial technically met its primary endpoint, showing the LAAC device was non-inferior to anticoagulation— based on pre-defined safety and efficacy margins. While technically positive, The CHAMPION trial was met with tempered enthusiasm, particularly because there was a numerically higher rate of ischemic stroke in the device group than in the anticoagulation group.
On the other hand, bleeding outcomes clearly favored the device. Major bleeding—defined as critical, fatal, or transfusion-requiring bleeding, along with clinically relevant non-major bleeds requiring hospitalization or HCP intervention—was reduced by about 50%. This represents a meaningful advantage for LAAC.
When we consider net clinical benefit, we’re weighing a numerically higher—but statistically non-inferior—rate of ischemic stroke against an approximate 50% reduction in bleeding. The key question is whether that tradeoff justifies the procedural risk. That’s where the net clinical benefit argument becomes important.
This is particularly compelling for patients facing long-term anticoagulation. If someone is likely to be on a blood thinner for 20 years, the cumulative benefit may favor the device, we will see how the argument changes when the 5-year follow-up data is presented.
CHAMPION-AF used a modified definition of clinically relevant non-major bleeding. Can you comment on that definition and why it’s important in interpreting the results? Why are these types of bleeds still relevant for patients?
Trials like CHAMPION and OPTION set clearer guardrails around what counts as “clinically relevant” bleeding—generally requiring evaluation or treatment by a clinician, such as a visit to a doctor, nurse practitioner, or the emergency department. The idea was to use a higher threshold for defining meaningful bleeding events, focusing on events that may cause patients to stop taking their DOAC therapy.
I saw this in my own trial patients. Some had nosebleeds but managed them at home without intervention, so they didn’t stop anticoagulation and cross over to receive a WATCHMAN FLX device. That’s important, given criticism that LAAC trials use endpoints that are easier to achieve. The goal is to show that you can provide similar—or near-similar—ischemic stroke protection without the long-term consequences of anticoagulation. Tightening the definition of clinically relevant bleeding helped ensure a more meaningful endpoint and made crossover less likely.
It’s also notable that CHAMPION enrolled patients who were already tolerating and adhering to anticoagulation. Compliance was high—about 87% at 3 years—which exceeds real-world experience. In earlier anticoagulant trials, adherence dropped to around 70% by 18 months. In practice, patients often stop therapy due to bleeding, cost, dosing preferences, forgetfulness, or physician guidance. CHAMPION, by design, selected patients more likely to remain compliant, enriching the study population accordingly.
Given the evolving evidence base, how are you currently selecting patients for WATCHMAN implantation, and how will that shift in light of CHAMPION-AF?
I don’t think this will significantly change which patients I select for appendage closure—at least not yet. I’d like to see improved devices with lower rates of peri-device leak and device-related thrombus. Alternatively, I’m comfortable offering a device if the patient agrees to continue anticoagulation for 6-12 months post-implant and then stop once the device is fully healed. That’s part of why I don’t think we’re ready to use this as first-line therapy in patients who are content with anticoagulation.
In patients undergoing AF ablation—who are symptomatic, have moderate stroke risk, and possibly some increased bleeding risk—I do consider appendage closure, often in a concomitant approach. This was studied in OPTION, where ablation and closure were performed together (or staged by 3-6 months post ablation). If I’m already treating AF invasively, combining procedures in a single setting—with one anesthesia and one vascular access—can make sense, particularly for patients with CHA₂DS₂-VASc scores of 3, 4, or 5.
While some CHA₂DS₂-VASc 2 patients were included in CHAMPION and OPTION, I generally would not offer a device in this group based on recent results from the OCEAN and ALONE-AF trials.
What CHAMPION adds, in my view, is support for discussing LAAC as an option in patients who feel they are not doing well on anticoagulation, even without a major or clinically relevant bleed. It allows for a more informed conversation, balancing the slightly higher stroke rate with the device against the reduction in bleeding risk.
Which patient profiles stand to benefit most from earlier consideration of LAAC?
It really comes down to time horizon and 2 probabilities: how long a patient will need to remain on anticoagulation, and the likelihood of progressing from intermittent to persistent or permanent AF. Most stroke protection studies—outside of OPTION, which focused on ablation—show that stroke risk increases once patients develop persistent or permanent AF, even if they remain on anticoagulation.
In terms of who may benefit most, 2 groups stand out: younger patients with an AF-related embolic stroke, and patients with CHA₂DS₂-VASc risk factors who have progressed to permanent AF. Of course, patients with a contraindication to anticoagulation already have a Class 2A guideline recommendation for appendage closure. But here we’re really talking about patients who tolerate anticoagulation—yet have had a stroke or have progressed to permanent AF—where closure could offer additive protection with relatively low procedural risk.
Procedural safety has improved considerably. In CHAMPION, OPTION, and PINNACLE FLX, complication rates were low, with pericardial effusion rates around 0.5% or less and no reported device embolization. As the procedure continues to get safer, the potential net clinical benefit will likely expand.
CLOSURE‑AF also generated significant attention with its comparison of LAAC to medical therapy. How do you interpret those findings alongside CHAMPION‑AF, and what should clinicians take away when looking at both studies together?
CLOSURE-AF intentionally enrolled a much higher-risk population than CHAMPION, with patients averaging a HAS-BLED score of 3 and a CHA₂DS₂-VASc score of 5. These were individuals already at significant bleeding risk if placed on anticoagulation. They were randomized to best medical therapy—which could include anticoagulation depending on rhythm status—or appendage closure using any available device.
The trial was conducted in Germany, with about half of patients enrolled by just 3 operators, so a small number of centers contributed most of the data. Device use was mixed: roughly 40% Amulet (Abbott), 40% WATCHMAN FLX, and about 20% WATCHMAN 2.5 or LAmbre.
A key issue in CLOSURE-AF was the strategy of stopping anticoagulation immediately after implantation and switching to dual antiplatelet therapy (DAPT) with aspirin and clopidogrel. I think that approach has largely been debunked, though it hasn’t fully translated into practice. In the randomized ANDES trial, device-related thrombus was nearly 3 times higher with DAPT compared to anticoagulation alone, and postprocedural bleeding was about twice as high, suggesting this is not an optimal post-implant strategy.
In CLOSURE-AF, I think these factors—higher-risk patients and suboptimal post-implant therapy—contributed to the negative result, where medical therapy outperformed the device. However, the broader body of evidence still shows less bleeding with appendage closure compared with medical therapy. That said, CLOSURE-AF is an independently conducted randomized trial and should not be ignored. It underscores the importance of careful patient selection and optimizing early post-implant management to reduce complications in the first months after the procedure.
Comparing the OPTION and OCEAN trials, what are key considerations regarding study design, patient populations, and the clinical questions being answered by each trial that are most important for clinicians to understand, and how do those differences influence how the data should be applied in practice?
OPTION had a higher CHA₂DS₂-VASc score, but both OPTION and OCEAN enrolled patients with relatively low HAS-BLED scores. In OPTION, about 40% of patients underwent ablation and device implantation essentially on the same day. In contrast, in OCEAN, all patients had been ablated at least one year before enrollment, so there was a delay before deciding on long-term therapy.
OCEAN compared rivaroxaban 15 mg with aspirin and was particularly informative because all patients underwent brain MRI before and after, allowing detection of both clinical and covert strokes. The results showed no meaningful difference in stroke outcomes between groups, but more bleeding—and slightly more intracranial hemorrhage—occurred with rivaroxaban over time.
This highlights an important issue for younger patients who may otherwise remain on lifelong anticoagulation: the ongoing risk of bleeding, including potentially fatal intracranial hemorrhage. That risk can potentially be reduced either by effectively eliminating AF with ablation, as in OCEAN, or by closing the appendage at the time of ablation, as in OPTION.
In practice, OCEAN helps guide decisions for lower-risk patients (eg, CHA₂DS₂-VASc ≤2), suggesting anticoagulation can be stopped after successful ablation with careful follow-up. However, for patients with CHA₂DS₂-VASc scores of 3 or 4—especially those at higher risk for AF recurrence post-ablation—stopping anticoagulation may be less appropriate. These patients may be better aligned with an OPTION-type strategy.
With appendage closure, if a patient remains stable for a year and stops anticoagulation, even if AF recurs later and goes undetected, their stroke risk is likely lower. In contrast, a higher-risk CHA₂DS₂-VASc 4 patient who undergoes ablation alone, stops anticoagulation, and later develops asymptomatic AF could present with a stroke. In that sense, OPTION and OCEAN address slightly different patient populations, but both provide useful guidance for managing patients undergoing AF ablation.
How do trials like CHAMPION‑AF shape conversations with patients on NOAC around stroke protection options, particularly when balancing risks and benefits from available therapies?
There is a clear net clinical benefit argument—reducing bleeding while maintaining reasonably good stroke protection. This allows for a meaningful discussion with patients, supported by solid data. Having these studies published in the New England Journal of Medicine is helpful, as many patients recognize and trust that source. I often review the articles with them in clinic, even printing them out so they can consider the data at home.
I’m open to considering this on a case-by-case basis, and it certainly helps facilitate conversations between referring physicians and implanters. You’ll still see variability—some implanters have a lower threshold to offer the device, while some referring physicians remain hesitant. There is ongoing debate and differing levels of acceptance, reflecting the reality that there is no one-size-fits-all approach to stroke protection in AF, and no one size fits all perfect device for every LAA.
The transcripts have been edited for clarity and length.
Disclosures: Dr Ellis has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports he is an advisor/consultant for Abbott, Boston Scientific, Conformal Medical, and Medtronic. He is also on the steering committee for the CLEAR Study (Abbott), Watchman Elite (Boston Scientific), the VERITAS Study (Abbott), and CONFORM IDE Trial for the Conformal CLAAS AcuFORM System (Conformal Medical).
This content was published with support from Boston Scientific.
WATCHMAN FLX Pro LAAC Device- Implanter- Indications, Safety and Warnings


