

Sterile V1 Electrode Placement for the Extraction Environment
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2025;25(10):24-25.
Ryan J Donovan, PA-C; Nimrod Lavi, MD; and Eric Bader, MD
Yale Electrophysiology
Transvenous lead extraction is a cornerstone of any successful lead management program. With the advent of conduction system pacing (CSP) as well as emerging evidence of its clinical superiority, it has become necessary to offer and utilize this technique for reimplantation following lead extraction. Successful CSP often utilizes a 12-lead electrocardiogram (ECG), or at a minimum, leads V1 and V6, to confirm appropriate pacemaker lead location. However, when extraction is performed in a traditional operating room/cardiothoracic (CT) surgery environment, patients are sterilely prepared for possible rescue via emergent open heart surgery. There are limitations involved with adding a nonsterile electrode to the sterile surgical field and prepping in a sterile fashion over this, should rescue need to be performed. This provided us the opportunity to create a method of establishing a sterile V1 ECG electrode. Presented here is a method for establishing this sterile lead by adapting epicardial pacing leads and pacing cables traditionally utilized in CT surgery.
Methods
First, the limb lead stickers RA, LA, RL, and LL are connected to the patient with standard nonsterile adhesive electrodes. Similarly, V6 and possibly V5 can be attached with nonsterile adhesives in the usual locations since these are lateral to the sterile field. The ECG machine should also be positioned in such a manner that it can be easily visualized at the time of reimplant.
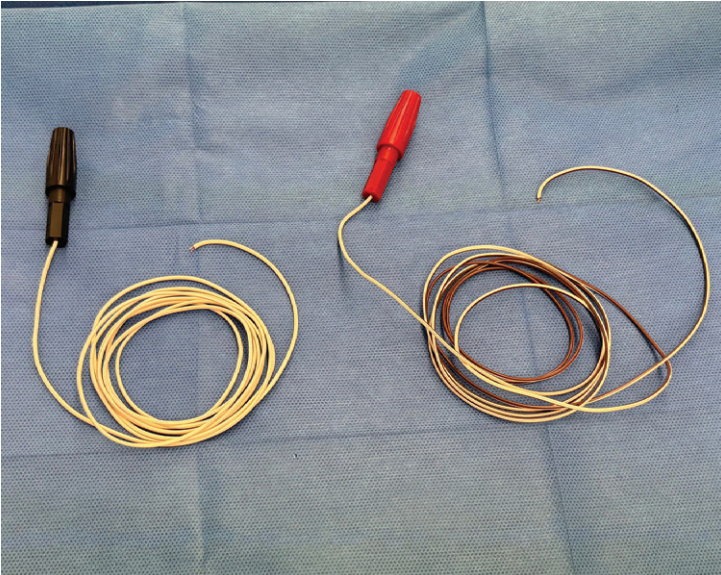
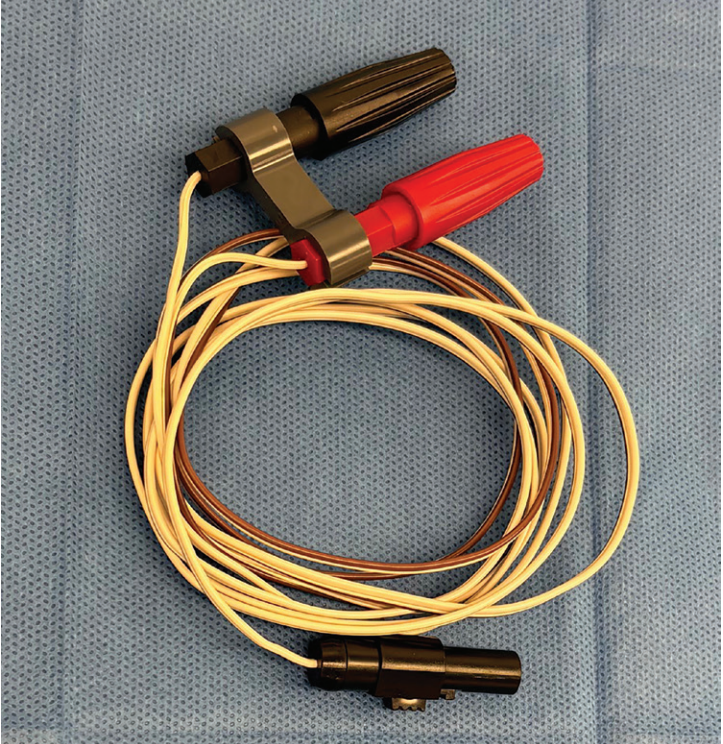
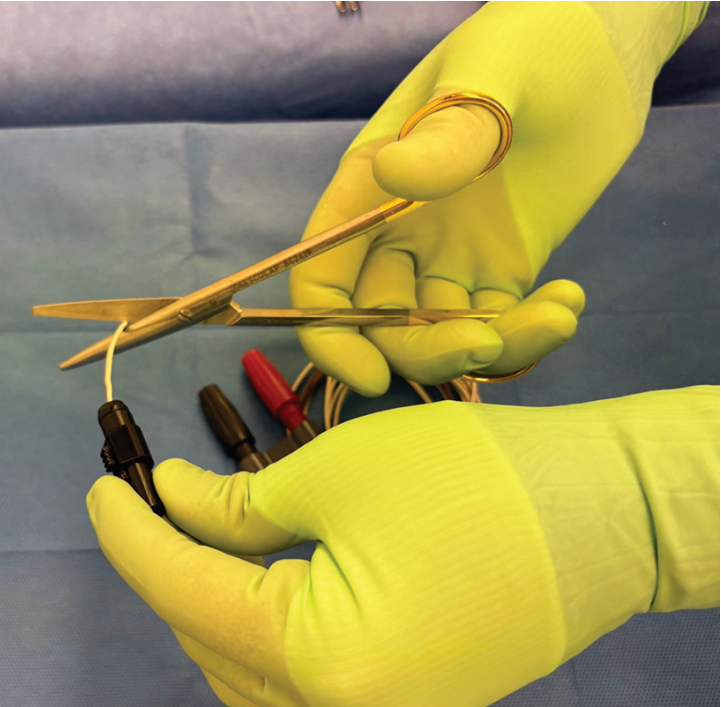
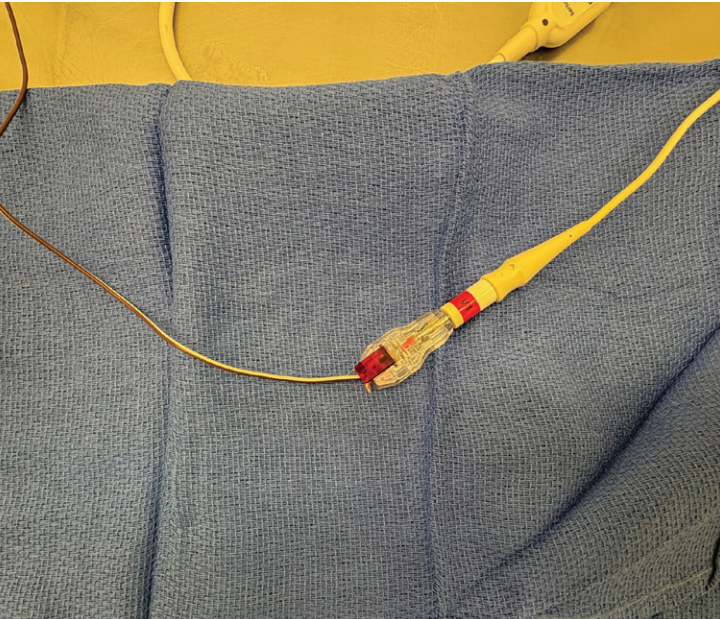
Prior to draping the surgical field, the sterile cardiac surgery epicardial pacing connector cables (Figure 1) are prepared as in-line extensions for the V1 electrode. This is easily done on the sterile table. The scrub technician separates the distal connector (Figure 2) and divides the 2 cables into 2 separate pieces (Figure 3), and one cable is passed off the sterile field. A short (approximately 2-cm) section of the conductors of this cable is exposed (Figure 4) and inserted into the V1 clip of the ECG machine (Figure 5). For conductor exposure, a traditional electrician’s wire stripping device is used, but alternatively, scissors as well as scalpel blades can be carefully utilized.

Once connected to the ECG machine, the connector can be left disconnected in place, where it can be easily connected at the time of reimplant after extraction is safely completed. The other half of the connector cable is kept on the surgical field until the time of reimplant. It is to be used as a “sterile to nonsterile” extension between the sterile V1 electrode and nonsterile pacing cable extension previously connected to the ECG machine.
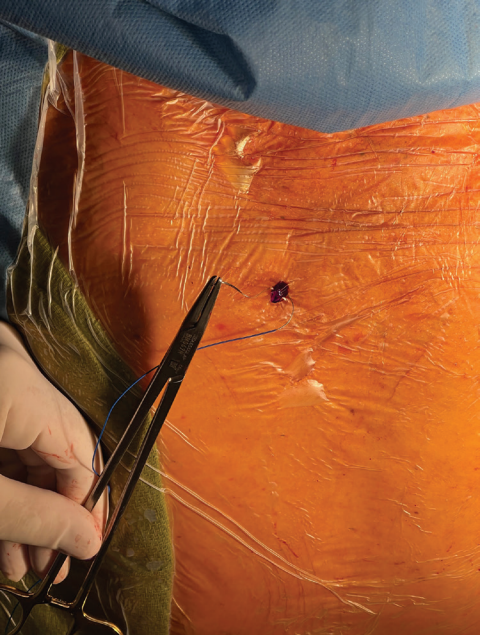
At the time of reimplant, with the chest prepared in the traditional sterile fashion, an epicardial pacing needle is placed into the skin at the standard V1 position and secured (Figure 6). The distal sharp needle end of the pacing needle is then divided, and the remaining pin is inserted into the connector cable (Figure 7), which has been kept on the sterile field and is
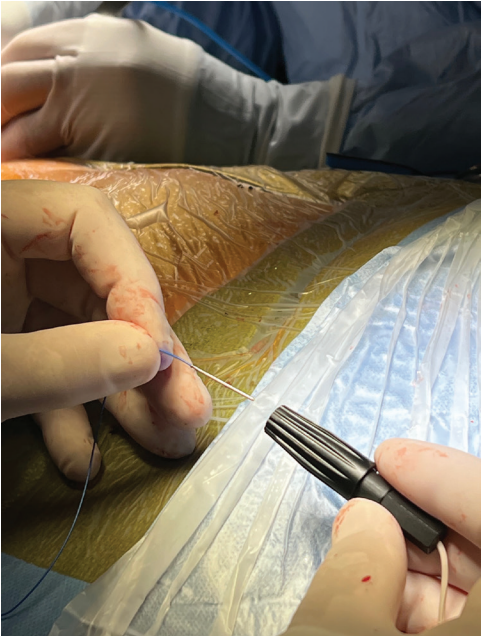
also secured to the field. The other end of this cable is then passed off the field and prepared in a similar fashion to its mate, by stripping off the distal 2 cm of insulation. The exposed and now nonsterile conductors can be inserted into the connector end of the other nonsterile connector cable (Figure

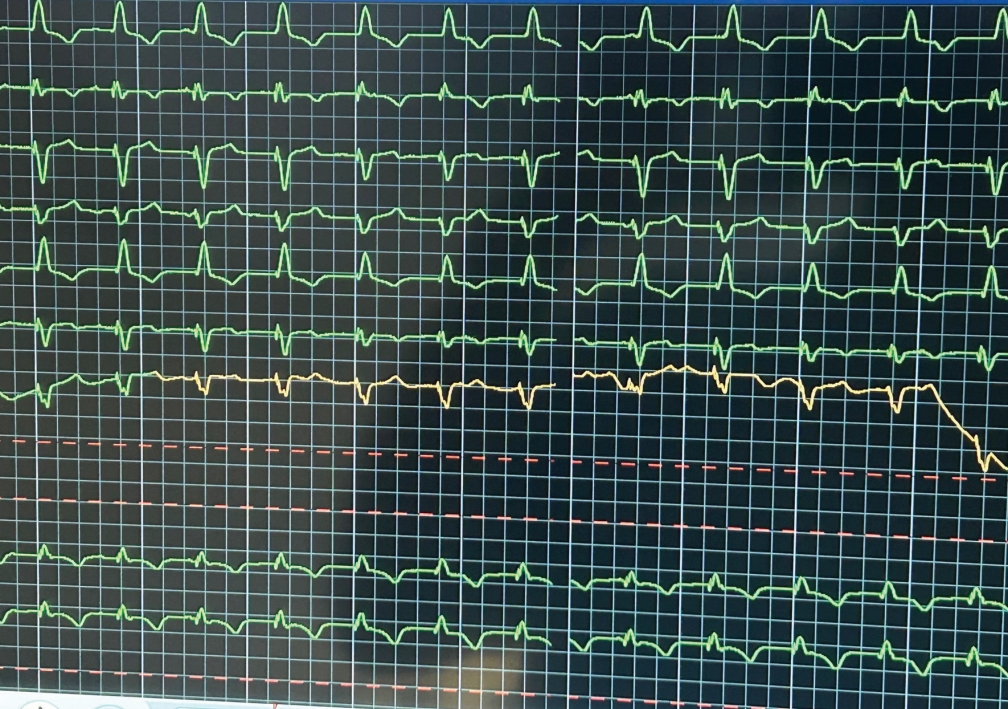
8). This will then complete the V1 electrode. If desired, the same steps could be undertaken for V2, V3, and/or V4, but in our experience, V1 and V6 have been satisfactory for confirmation of left bundle branch signal in this environment (Figure 9).
Conclusion
The benefit of CSP has been demonstrated in appropriately selected patients. Successful CSP is contingent on having precordial leads available to review intraoperatively. This report presents a practical method for applying sterile leads during an extraction without compromising sterile technique or surgical outcomes. By adapting epicardial pacing leads and cables, this technique enables reliable CSP implementation, supporting safer and more effective reimplantation strategies.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Nimrod Lavi, MD, and Eric Bader, MD, have no disclosures to report. Ryan J Donovan, PA-C, reports consulting fees, payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events, payment for expert testimony, and support for attending meetings and/or travel, from Philips.

