

Endocardial Ablation of the Left Atrial Ridge for Treatment of a Marshall Bundle Tachycardia
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(3).
Tobias Ahnert1; and Ankit Maheshwari, MD2
1Noorda College of Osteopathic Medicine, Provo, Utah; 2Pennsylvania State University Milton S Hershey Medical Center, Hershey, Pennsylvania
The left atrial (LA) ridge is a fold of tissue separating the left pulmonary veins (PVs) from the left atrial appendage. It contains the ligament of Marshall, and its components include the vein of Marshall, autonomic nerve ganglia, and Marshall bundle (MB). The MB has discrete connections with the muscle sleeves of the coronary sinus and PVs as well as the LA.1,2 This complex network can serve as a substrate for re-entry and arrhythmias including atrial fibrillation (AF) and organized atrial tachycardias. Described here is a case of successful ablation of a MB tachycardia.
Case Presentation
A 59-year-old man presented for ablation of atrial tachycardia, which developed 5 months after AF ablation with pulmonary vein isolation (PVI). An electroanatomic map was created using the Carto system (Johnson & Johnson MedTech) and Octaray catheter (Johnson & Johnson MedTech). The PVs remained chronically isolated. During atrial tachycardia (Figure, A), the LA was activated from a focus inferior to the left inferior PV, a region previously described to harbor insertions of the MB.2,3 The entire tachycardia cycle length was not accounted for by mapping the endocardial LA surface. Long, low-amplitude fractionated potentials (*, †) were noted along the LA ridge (dotted line). A MB tachycardia was suspected and the ridge was ablated from both sides (QDOT Micro, Johnson & Johnson MedTech). Ablation at the superior region of the ridge (*) resulted in slowing of the tachycardia (Figure, B) and subsequent degeneration into AF (Figure, C). The tachycardia was re-induced after cardioversion of AF and was successfully terminated (Figure, D) and rendered noninducible by ablation from the middle of the ridge in the anterior carina (†). The patient remained arrhythmia free after 8 months.
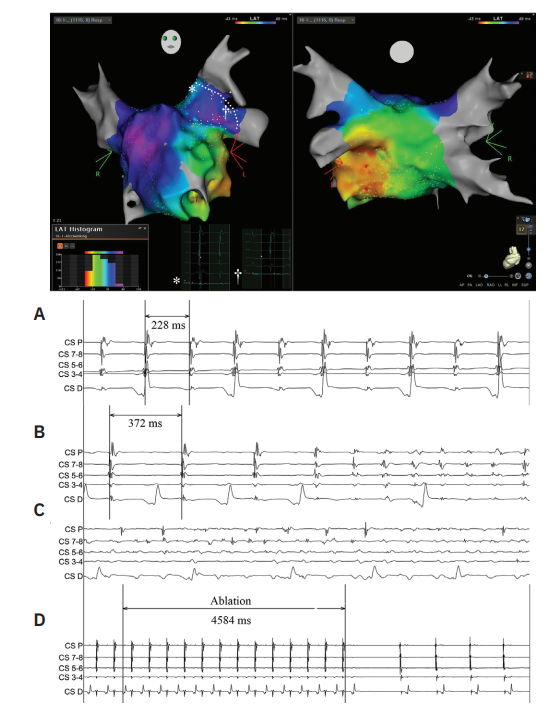
Abbreviations: CS, coronary sinus; D, distal; LAT, local activation time; P, proximal.
Discussion
Additional ablation of the LA ridge beyond what is needed to achieve electrical isolation of the PVs can facilitate endocardial MB ablation for treatment of MB arrhythmias. The MB network has been implicated in PVI failure and post-PVI atrial tachycardias.2 Targeting the MB with ethanol infusion into the vein of Marshall has been shown to improve arrhythmia-free survival after PVI.4 Future studies should investigate whether additional endocardial ablation of the LA ridge after PVI to empirically target the MB can reduce post-PVI atrial arrhythmias.
Summary
Recognizing patterns of LA activation during MB tachycardias can aid in diagnosis and treatment planning. The MB can be successfully targeted by ablation of the LA ridge from the endocardium, which may reduce the rates of post-PVI arrhythmias.
Funding: No internal or external funding was used for this manuscript.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Tobias Ahnert reports employment by Johnson & Johnson from April 2020 to June 2025, and reports stock in Johnson & Johnson. Ankit Maheshwari, MD, has no conflicts of interest to report.
References
- Tanaka Y, Takahashi A, Yano H, et al. Clinical and electrophysiological characteristics of Marshall bundle–related atrial tachycardia: considerations based on a definitive diagnosis. JACC Clin Electrophysiol. 2025;11(2):362-372. doi:10.1016/j.jacep.2024.10.019
- Chee J, Kalogeropoulos AP, Almasry I, et al. Identification and endocardial ablation of the ligament of Marshall for pulmonary vein isolation. JACC Clin Electrophysiol. 2021;7(3):283-291. doi:10.1016/j.jacep.2020.08.027
- Ahnert T, Maheshwari A. Burning bridges: ablation of a bi-atrial macro-reentrant tachycardia conducting via Bachman’s bundle and the Marshall bundle complex. Indian Pacing Electrophysiol J. 2024;24(1):40-41. doi:10.1016/j.ipej.2023.11.001
- Valderrábano M, Peterson LE, Swarup V, et al. Effect of catheter ablation with vein of Marshall ethanol infusion vs catheter ablation alone on persistent atrial fibrillation: the VENUS randomized clinical trial. JAMA. 2020;324(16):1620-1628. doi:10.1001/jama.2020.16195

