

Comprehensive Atrial Fibrillation Management in a Concomitant Case: A Combined FARAPULSE™ PFA Platform and WATCHMAN™ Left Atrial Appendage Closure Workflow
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(6):6-7.
Nicholas Olson, MD, FHRS
Scripps Health, La Jolla, California
For patients with persistent atrial fibrillation (AF), typical atrial flutter, and elevated stroke risk who cannot tolerate long-term anticoagulation, addressing each problem independently across separate procedures introduces unnecessary risk, resource burden, and patient inconvenience. In this case, we describe a combined workflow utilizing the FARAWAVE™ NAV Catheter (FARAPULSE™ PFA Platform, Boston Scientific) for pulmonary vein isolation (PVI), the FARAPOINT™ Catheter for cavotricuspid isthmus (CTI) ablation, and the WATCHMAN FLX™ Pro Left Atrial Appendage Closure (LAAC) Device for LAAC procedures—all performed in a single lab visit with a shared transseptal access.
PVI With Contact-Sensing Mapping
Following transseptal puncture using the FARADRIVE™ Steerable Sheath under fluoroscopic guidance, the FARAWAVE NAV catheter was introduced and opened in the flower configuration. The catheter was rotated mid-chamber to establish a blood pool baseline impedance—a step we perform routinely before mapping to establish a reliable reference for tissue contact detection.
A baseline voltage map of the LA was then obtained using the FARAVIEW™ Software Module on the OPAL HDx™ Mapping System (Boston Scientific). The LA volume measured 27.61 cc on electroanatomic reconstruction.
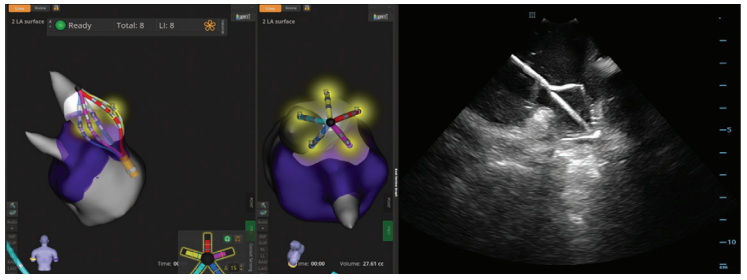
Contact sensing on the FARAWAVE NAV catheter uses local impedance measurements to confirm tissue engagement, adjunctive to other visualization methods, for catheter positioning (Figure 1). We rely on these impedance changes—rather than fluoroscopy alone—to confirm tissue engagement before each energy delivery. Visualizing adequate contact across all 5 petals simultaneously with a single intracardiac echocardiography view is often challenging, particularly at the posterior wall and roof; contact sensing provides a complementary layer of real-time information that reduces ambiguity and helps identify potential gaps before they become reconnection sites.
Projected PFA markers (FIELDTAG™ Technology, Boston Scientific) were displayed during positioning to provide a continuous visual guide for circumferential coverage. PVI was completed without catheter exchange or introduction of additional sheaths. The single catheter map-and-ablate approach is central to why we have adopted this workflow—it reduces access complexity and procedural steps while maintaining diagnostic fidelity throughout the case.

CTI Ablation: A Structured, Protocol-Driven Line
Upon completion of PVI, attention shifted to CTI ablation for typical flutter. We chose to address the CTI within the same procedure for 2 reasons: the patient had documented flutter on presenting rhythm strips, and performing CTI ablation immediately after PVI—while the patient remains anticoagulated and access is established—avoids a return visit and a second procedure entirely. The right atrial volume measured 18.54 cc on reconstruction (Figure 2).
The FARAPOINT PFA Catheter was advanced to the right atrium and positioned along the CTI under fluoroscopic guidance. We ablated 8 discrete sites along the isthmus, delivering 2 applications per site. At the site nearest the tricuspid valve annulus, we delivered 3 applications—this region carries higher risk for incomplete lesion formation given tissue thickness and trabeculation at the annular insertion, so additional energy at that anchor point is part of our standard approach. Total applications on the CTI line were 17.
This protocol aligns with the ADVANTAGE AF Phase II best-practice framework of 2 applications per site targeting 3- to 5-mm spacing to ensure overlapping lesions, with deliberate titration on the annular site based on local anatomy. Fluoroscopic catheter positioning, coupled with FIELDTAG Technology PFA markers, guided placement at each site along the isthmus line. To reduce the risk of coronary vasospasm, nitroglycerin boluses (3 mg initial, 2 mg every 2 minutes) can be administered into the right atrium.
Left Atrial Appendage Closure: Completing the Case
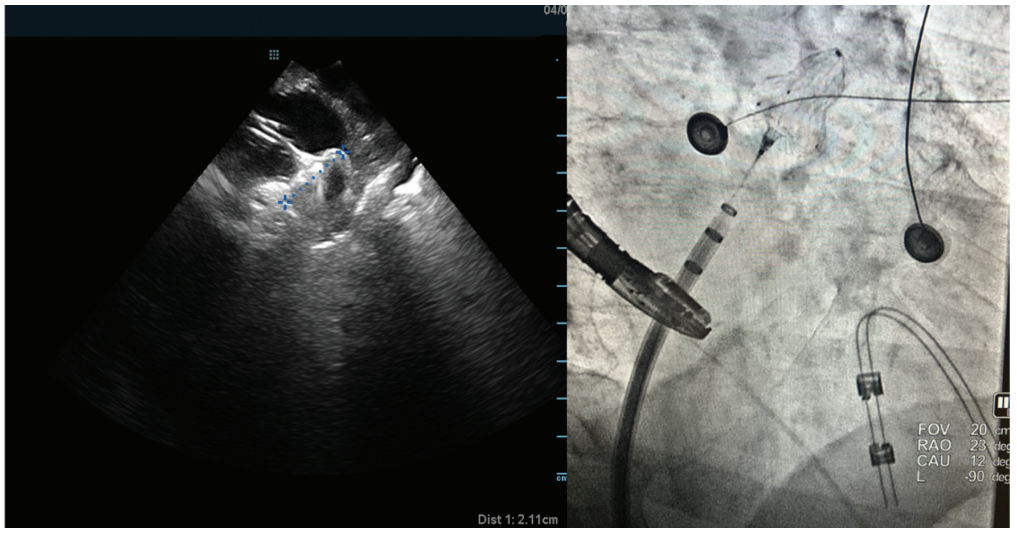
With rhythm management complete, we transitioned to WATCHMAN FLX Pro implantation without terminating access. The established transseptal sheath position simplified catheter exchange to a WATCHMAN TruSteer delivery sheath, eliminating the need for a new access step. The transesophageal echocardiography (TEE) probe was maintained in position from the ablation portion of the procedure. TEE-guided sizing revealed a 2.11-cm LAA ostial diameter measured pre-ablation, with device selection based on standard sizing protocol targeting appropriate compression range.
Fluoroscopic positioning was confirmed at RAO 23°/CAU 12° (Figure 3). Device deployment proceeded with stable positioning verified across all standard release criteria—PASS criteria confirmed, with no peri-device leak on final Doppler imaging. Apixaban 5 mg twice daily was administered peri-operatively and will continue for 3 months post procedure. The rationale for combining LAAC in the same procedure is straightforward: this patient had a documented contraindication to long-term anticoagulation. Achieving both electrical and mechanical stroke prevention in a single procedure reduces cumulative procedural risk and simplifies postprocedural anticoagulation management from day one.
A Single-Session Solution for a Complex Patient
This combined workflow demonstrates that FARAPULSE PFA and WATCHMAN FLX Pro implantation can be completed efficiently in a single streamlined case. Contact sensing capability on the FARAWAVE NAV catheter was central to the PVI portion of the case, enabling confident tissue engagement assessment throughout mapping and ablation. For the CTI, a structured fluoroscopy-guided protocol with deliberate site selection and application titration, supported by FIELDTAG Technology, produced a complete isthmus line without the need for additional imaging adjuncts.
For appropriately selected patients who require rhythm management and stroke protection and who cannot tolerate long-term anticoagulation, this approach offers a clinically complete procedure-efficient solution in a single lab visit.
Disclosures: Dr Olson has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports support from Boston Scientific for the manuscript (medical writing/editing <10% and article processing charges). He also reports consulting fees and honoraria from Boston Scientific for lectures, presentations, and educational events.
This content was published with support from Boston Scientific.

