


Angelina Collins, MSN, on STRIDE II and Treat to Target
Nurse practitioner Angelina Collins reviews the use of the STRIDE II guidelines for implementing treat to target therapy among patients with Crohn's disease.
Angelina Collins, ANP-BC, is an advanced practice provider specialist in the treatment of patients with inflammatory bowel disease at the University of California San Diego.
CLINICAL PRACTICE SUMMARY
Treat-to-Target in Adult Crohn’s Disease (STRIDE-2 Consensus Framework, US Care Setting)
- STRIDE-2 recommendations, not guidelines for adult outpatient care for inflammatory bowel disease (Crohn’s disease and ulcerative colitis) emphasize goal setting at every visit and shared decision-making. Clinicians should define patient-specific targets (e.g., bleeding, urgency, weight regain, functional goals like travel or events) and reassess at each encounter with frequent monitoring to guide therapy adjustments.
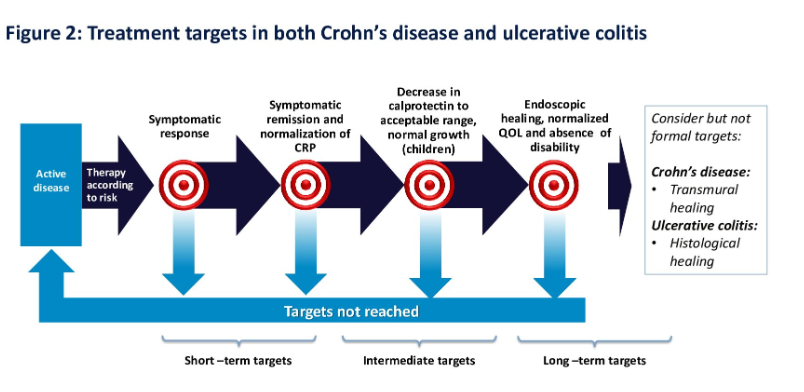
- Risk-based therapy selection and defined response timelines are central. Treatment choice should reflect current disease activity/severity (symptoms, endoscopy, radiology) and prognosis (including extraintestinal manifestations and complications). Expected symptom response occurs in days or weeks, varying by line of therapy. Patients treated earlier with an advanced therapy in their disease course may respond faster than those who have already been exposed to multiple therapies.
- Objective targets and monitoring timelines include symptomatic remission and biomarker normalization within 3–6 months; endoscopic healing ~6 months. Targets include improvement/normalization of CRP and reduction in fecal calprotectin if it was elevated at baseline. Ongoing long-term monitoring is required; if targets are unmet, consider optimization or add/switch therapy. Avoid undertreatment due to risk of long-term complications in this chronic disease.
TRANSCRIPT
Hi, I'm Angelina Collins. I'm a nurse practitioner at the Inflammatory Bowel Disease Center at the University of California, San Diego. I specialize in caring for adults with Crohn's disease and ulcerative colitis. So the discussion today on treat to target and using the STRIDE-II consensus is going to focus on adult patients. Keep in mind, the STRIDE-II are recommendations. They're not guidelines, but they're recommendations on how to approach patient management and how to think about treating to a target.
But really the question becomes, how do you do this in real time? So what I like to do is I think about this as a framework that can guide our visits and goals of care. First and foremost, I think it's really important to think about evaluating this every time you're seeing a patient at every visit. What I think is really important is for you and your patient to establish your goals. I'd suggest thinking about what's the most burdensome or troublesome part of what is happening to your patient? What part of the disease process is most frustrating? Is there a symptom you want to have in mind and measure as is improved over time? Is it bleeding? Is it urgency? Is it the ability to regain lost weight? What are they missing that they might like restored? Are they missing the confidence in travel or ability to attend a baseball game? Is there a big event that's coming up that they'd like to be able to be well for? And then plan to keep in mind that at every time you're seeing the patient, you're going to be planning for frequent re-evaluations and monitoring to ensure that things are moving smoothly along the pathway. I like to introduce this at the very beginning of the visit, and I like to introduce this early on because this is really going to continue throughout all the visits that you'll be seeing them.
So then you want to think about selecting the appropriate therapy according to risk, which really means that you're thinking about both disease activity and severity. So think about how sick your patient is right now, and that would be based on their symptoms, on endoscopy, on radiology, but then also think about their prognosis and maybe also think about extraintestinal manifestations or how the disease is affecting them globally. How sick are they and what is that going to lead to?
And then you really want to consider the timeline for which you expect people to have a response. So when you think about symptom response, and this means overall improvement, this might be days or weeks depending on the therapy selected and prior treatments that they've been on. That's an important concept because we might think about patients who are on their first line of treatment, maybe responding a little bit earlier than if this was, say, maybe their fourth therapy.
The next part is symptomatic remission, and that's feeling well. So this is also the time to expect CRP, if it was evaluated at baseline or elevated at baseline, to normalize. Think about fecal calprotectin. Again, if it was elevated at baseline, this should be improving and reducing to the acceptable range. So you want to be thinking about this and what is your target? Is it maybe the fecal calprotectin to be less than 250? Is it less than 150? Is it less than 50?
And we should expect all of those to be happening within 3 to 6 months. And then for endoscopic healing, meaning improvement, first, remember you've got to look. If you don't look, you don't know. So it's really important to set that expectation up at the beginning with your patient. And thinking about the timing of this is likely going to be somewhere around the 6-month mark from the start of therapy, might be a little bit longer depending again on how many other therapies your patient has previously been on.
So I generally frame all of this at the first visit and when selecting therapy. So I tell my patients in really simple terms that my goals for you are to feel well; I want to have healing of the inflammation; I want to prevent complications, and that means both complications from the disease, but also complications from any medication therapy or management strategy that we're going to choose. They are often really concerned about this, and so they're thinking about that as first and foremost. But I think for those of us that are on the provider side of things, we really know that there's a real risk in overtreating our patients, but there's probably a bigger risk in undertreating patients, that smoldering disease that leads the way to long-term complications.
And then I want you to think next, it's not really going to stop there at the 6-month mark or the 1-year mark. Remember, this is a chronic disease that requires long-term monitoring and management strategies. So once you've hit your targets and you hopefully have hit those, then great, then you're going to continue on that for long-term monitoring and management. And if you haven't hit those, then you're going to be thinking about maybe you need to give a little bit of extra time, maybe you need to be optimizing, maybe you're adding, maybe you're switching as appropriate.
And then again, you're going to keep going. So the SPIRIT consensus, which I think in general doesn't really get enough attention and maybe not the attention it deserves. It's really focusing on and highlighting that this is, again, a chronic disease that we are managing, and the goals of care are going to continue over time.
So early diagnosis, appropriate treatment selection early in the disease course can really change the long-term disease course and change your prognosis and change what's going to happen for people in the end. So I think that's really an important part of things. And I think it's also doubly important to be thinking about that not only are we doing this while we are managing, maybe we think about a medication strategy, but this should be our same management strategy no matter what kind of therapy our patients are suggesting. If they're following a diet therapy, you still follow this. If you're following a naturopathic therapy, you're still going to follow this. And it's really important for our patients to know and understand that we're going to support them and walk with them as they are selecting their management strategy, and we're going to use the same goals of care and the same treatment guidelines no matter how we do it.
Thank you so much for joining me today. I really appreciate your time.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the AIBD Network or HMP Global, its employees, and affiliates.
Related Content

The NP/PA Institute is dedicated to educating and informing advanced practice providers on clinical topics and practical issues to support the profession and improve the quality of care for patients with inflammatory bowel disease (IBD).
The AIBD NP/PA Institute is designed for Advanced Practice Providers who specialize in Inflammatory Bowel Diseases, to further their education and increase their knowledge to achieve better patient outcomes. Explore cutting-edge research, innovative treatment options, and new therapeutic methods, while remaining focused on the fundamental principles and terminology associated with IBD.
October 17-18, 2026 | New York | Register Now
November 12-13, 2026 | Virtual | Register Now
