Reframing Generalized Pustular Psoriasis: From Pathogenesis to Early Clinical Intervention
At the Fall Clinical 2025 session, “Shifting the Management Paradigm in Generalized Pustular Psoriasis,” presenters Raj Chovatiya, MD, PhD, and Boni E. Elewski, MD, outlined the evolving understanding of generalized pustular psoriasis (GPP) as a distinct disease entity, both in its immunologic underpinnings and its clinical implications. The session emphasized how early recognition, knowledge of trigger factors, and prompt dermatologic intervention can significantly alter outcomes in what remains a life-threatening, often misdiagnosed condition.
GPP is increasingly recognized as a genetically distinct, autoinflammatory disease, rooted in innate immune system dysfunction. Dr Elewski began by recounting a 2011 New England Journal of Medicine study that identified a mutation in the IL-36 receptor antagonist among several Tunisian families with autosomal recessive GPP. The absence of this antagonist results in unchecked activation of the IL-36 receptor and a cascade of downstream inflammatory cytokine production, particularly driving neutrophilic inflammation.
“This was a very nice, clean story,” she said, “from the bench to bedside,” referencing the fact that the first targeted treatment for IL-36–driven GPP was approved just 11 years after the genetic mechanism was first described.
Dr Chovatiya added that IL-36 plays a critical role in the innate immune response, differentiating GPP from plaque psoriasis, which is more adaptive immunity-driven and primarily associated with the IL-23/IL-17 axis. Although IL-36 is also overexpressed in plaque psoriasis, its role is amplified in GPP and contributes to crosstalk between pathways, making the 2 conditions related yet distinct.
“We really think of GPP as truly an innate immune-driven disease,” Dr Chovatiya explained. “In the case of plaque psoriasis, it's much more of an adaptive immune-driven disease.”
GPP can present in a spectrum of severity but often follows a relapsing-remitting course marked by acute flares. While the term “generalized” may imply full-body involvement, Dr Elewski clarified that GPP does not need to affect every square centimeter of skin. Instead, it must involve more than 1 non-acral area, such as the leg and arm, to qualify. That distinction is important for dermatologists who may dismiss more localized presentations as less severe.
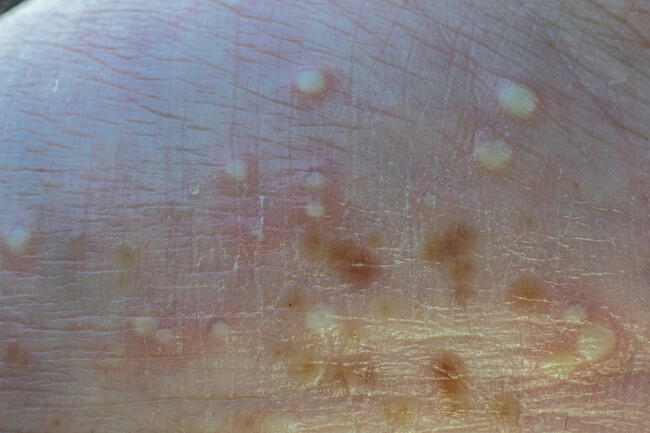
Dr Elewski described a critically ill patient she encountered in the ICU. “She was beet red. She had pustules. The small pustules coalesced into big pustules, what we call pustular lakes,” she said. The patient also had fever, leukocytosis, and systemic symptoms—hallmarks of severe GPP.
Systemic involvement in GPP may include elevated C-reactive protein, erythrocyte sedimentation rate, leukocytosis, and electrolyte imbalances, along with fever, malaise, and fatigue. Some patients may also present with arthritis, uveitis, or even cholangitis, highlighting GPP’s potential for multi-organ inflammation. “This is one of the few skin diseases that can have very severe systemic manifestations,” Dr Chovatiya stressed.
Although GPP flares are often spontaneous, identifying potential triggers is an essential part of disease management. Dr Elewski noted that systemic corticosteroids are 1 of the most frequent culprits in inducing flares and advised against their use in psoriasis patients. “I don’t like giving steroids to my psoriasis patients,” she said, sharing that even a single intramuscular steroid injection can provoke a full-blown GPP flare.
Other known triggers include hydroxychloroquine, beta-blockers, infections, and physical stressors such as sunburn or pregnancy. “The money is on drugs,” she emphasized, suggesting that dermatologists conduct a deep dive into the patient’s recent medication history. One anecdote described a patient who developed GPP after taking hydroxychloroquine during travel to a malaria-endemic region—a stark reminder of the importance of reviewing medication contraindications.
GPP is frequently misdiagnosed in emergency and inpatient settings, often confused with sepsis or acute infections due to its overlapping features: fever, leukocytosis, systemic inflammation, and pustular skin findings.
“Imagine that patient presenting to the ED,” Dr Elewski said. “There’s an ED physician, and they see a patient with pus on their skin, a fever, shaking chills, and a white count of 20,000. What do you think they’re going to do? Vancomycin.”
This misstep is common—and potentially dangerous—leading to unnecessary hospitalizations, antibiotic exposure, and delays in appropriate therapy. Dr Elewski shared multiple encounters where patients with GPP had been started on vancomycin, only for dermatology to later confirm the diagnosis and discontinue antibiotics. Compounding the issue, she noted, vancomycin itself is a known trigger for linear IgA bullous disease, which can further complicate the clinical picture.
These anecdotes reinforce the message that dermatologists must lead the diagnostic process when GPP is suspected. “We need to make the diagnosis,” Dr Elewski urged.
Patients with GPP face significant challenges, including unpredictable flares and poor quality of life. “Imagine looking like that, lying in bed, and thinking, What happened to me?’ Only to think it’s going to happen again,” Dr Elewski said.
Flares can occur multiple times a year and be debilitating. The psychological and emotional toll can be substantial, adding to the urgency of accurate diagnosis and timely intervention. In severe cases, GPP carries a reported mortality rate as high as 20% in the literature, underscoring the seriousness of untreated or mismanaged disease.
Because of the complex interplay of systemic inflammation, triggers, and innate immune dysfunction, GPP care often requires collaboration across specialties, including dermatology, rheumatology, and internal medicine.
Drs Chovatiya and Elewski emphasized several core takeaways for dermatologists:
- Understand IL-36-driven pathogenesis: GPP is fundamentally different from plaque psoriasis and requires distinct management.
- Recognize GPP early: It does not always present with full-body involvement but often includes systemic signs and pustular eruptions in multiple non-acral sites.
- Avoid corticosteroids: Systemic steroids are a well-known trigger for GPP flares and should be avoided.
- Review medication history carefully: Drugs like hydroxychloroquine, vancomycin, and beta-blockers can provoke disease onset or flares.
- Lead diagnosis and management: Dermatologists play a central role in identifying GPP, especially in hospital settings where the condition is commonly mistaken for infection.
- Act promptly: Misdiagnosis and treatment delays can lead to ICU admissions or even mortality.
The session closed with a clear message: Dermatologists must recognize GPP as a medical emergency and act decisively. By understanding its unique pathophysiology and potential severity, dermatologists can lead the way in reducing morbidity and improving outcomes for patients with this rare but life-threatening disease.
Reference
Chovatiya R, Elewski B. Shifting the management paradigm in generalized pustular psoriasis. Presented at: 2025 Fall Clinical Dermatology Conference. October 23–26, 2025; Virtual.