Revision Trapeziometacarpal Arthroplasty With Acellular Dermal Xenograft
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background: Osteoarthritis of the trapeziometacarpal joint is common. There are limited surgical options for patients who have undergone a failed primary trapeziometacarpal arthroplasty.
Methods: The authors conducted a retrospective review of patients who received a porcine dermal graft for failed trapeziometacarpal arthroplasty. Three hundred fifty-five trapeziometacarpal procedures were performed from 2005 to 2015; 9 were revisions. Seven were performed with xenograft interposition. Data included primary procedure, grip and key pinch strength, Visual Analog Score (VAS), motion, time to return to work, Kapandji Score, and radiographs.
Results: The mean follow-up was 84 weeks. The mean VAS score was 2.3, and all patients reported notable improvement. The mean Kapandji Score was 8. The mean grip was 20 kg, and the mean key pinch was 5 kg in the operated hand. The mean time to return to work was 12 weeks. The final radiographs showed improvement in spaces. No complications or immunological reactions were encountered.
Conclusions: The authors describe a technique for revision trapeziometacarpal arthroplasty with a porcine xenograft acellular dermal matrix. This technique shows a safe and valid treatment option with acceptable clinical outcomes.
Introduction
Trapeziometacarpal degenerative arthritis is a common condition seen in hand surgery and has been reported to symptomatically affect 25% to 33% of women and 10% of men.1,2 There have been a multitude of procedures described to treat patients primarily.1-6 The revision rate of trapeziometacarpal arthroplasty (TMA) is low overall and has been reported around 3% for soft tissue procedures.7 There are various etiologies of failure and need for revision; however, they have been reported mostly in reference to implant arthroplasty. This is usually due to loosening or instability, and revision rates from 3% to 16% have been reported in such cases.5,8,9 Revision of a joint replacement arthroplasty to a soft tissue procedure has been shown to have good results in decreasing pain and restoring some stability.5,10 The etiology of the continued symptoms or recurrence of symptoms after primary TMA with soft tissue procedures not involving implant arthroplasty is metacarpal subsidence, which can lead to thumb metacarpal-scaphoid or thumb metacarpal-index metacarpal impingement. This is known as mechanical failure and presents with loading pain, grinding, and instability.11 These cases are usually performed alone after a previous trapeziectomy or with ligament or tendon reconstruction.
A surgeon is faced with a difficult problem when TMA failure occurs and is left with limited options, which can vary based on the index procedure. Most revision procedures involve suspensionplasty techniques to bring the thumb metacarpal away from the scaphoid. These procedures include anchor, button, or all-suture suspension between the thumb and index metacarpals, tendon transfer alone, or a combination. These techniques may not fully address the impingement, especially between thumb and index metacarpals; thus, the development of other techniques that can address both subsidence and impingement issues is needed.
Various trapeziometacarpal interposition grafts, including acellular human dermal allografts, have been used with mixed results in primary arthroplasty procedures.1-3,6 Human allograft and xenograft have both been used in different areas of the body.12,13 Acellular dermal allografts are composed of donated cadaver tissue from which the cellular components have been removed while retaining the structural integrity of the collagen scaffold. Rendering the tissue acellular reduces the potential immunological risk of using porcine xenograft in human applications. Studies evaluating porcine xenograft use have shown mixed results regarding immunological reaction.12,14-15 Conexa (Tornier, Inc) is a porcine dermal matrix that has been demonstrated to be safe and effective in the clinical application of shoulder rotator cuff repair16 and has been shown to be load sharing in a biomechanical study.17
The purpose of this study is to report a new technique for treating failed TMA with porcine dermal matrix interposition in a distraction arthroplasty without suture or tendon suspension and to assess the clinical outcomes of patients. There are no current studies evaluating the use of porcine dermal matrix material as an interposition graft for revision TMA. The rationale for this study is to describe a surgical technique that can be an option for surgeons treating revision TMA and demonstrate that porcine dermal matrix is safe to use in the hand and wrist.
Surgical Technique
The operation is performed under a regional anesthetic block with or without intravenous sedation. A non-sterile tourniquet is placed on the upper arm, and standard sterile prep and drape is performed. A dorsoradial incision is made in a line from the distal radial styloid and carried distally toward the center of the thumb at the level of the proximal aspect of the first web space and trapeziometacarpal joint (Figure 1A). Care is taken to identify and protect the dorsal sensory branches of the radial nerve. The tendons of the abductor pollicis longus and extensor pollicis brevis are freed, and the interval between them is approached (Figure 1B). The radial artery is bluntly dissected, protected, and retracted from volar to dorsal. Arterial branches are coagulated as needed. An incision into the thumb trapeziometacarpal joint capsule in line with the skin incision is made. The space where the trapezium was previously located is inspected. Any existing areas of impinging bone or fibrosis are removed (Figure 1C). This is usually accomplished using a curved rongeur between the first and second metacarpals.
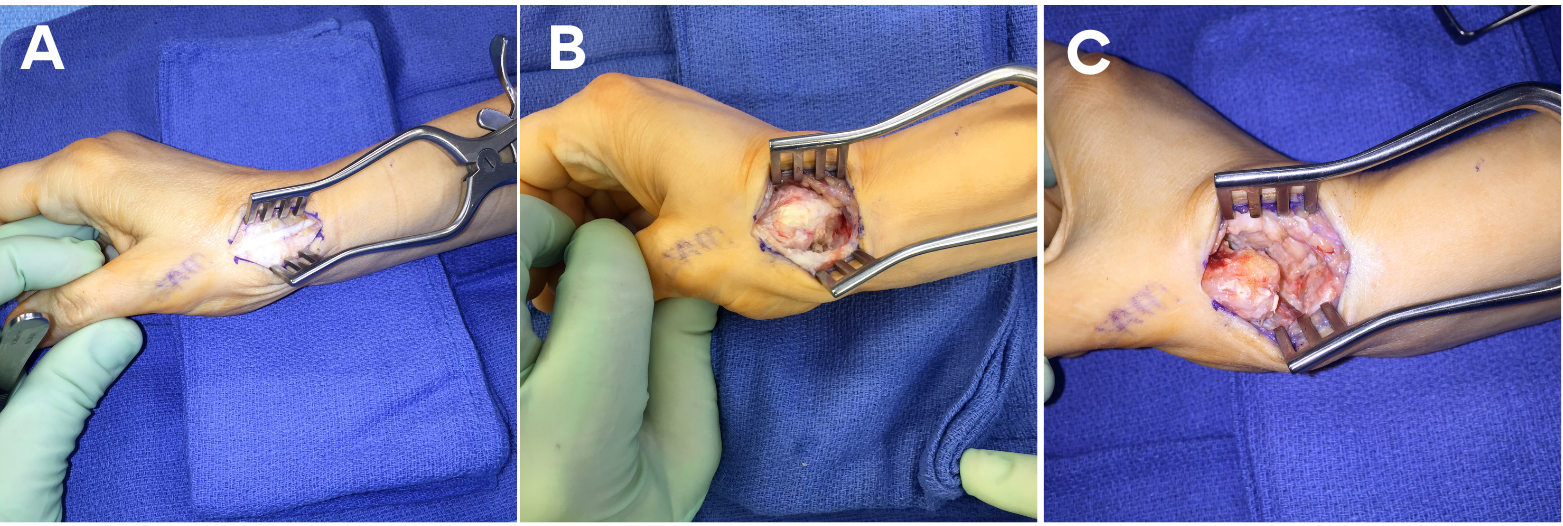
Figure 1. (A) Superficial surgical approach to the thumb carpometacarpal (CMC) joint. (B) Deep surgical approach to the thumb CMC joint. (C) The intermetacarpal and carpometacarpal space freed and prepared for graft.
An appropriately sized piece of Conexa graft is placed in sterile saline for 2 minutes; a 2 x 4-cm size is used in most cases (Figure 2A). It is then folded in half longitudinally, then folded in half again for appropriate thickness, and sewn together with 3.0 Vicryl sutures (Johnson & Johnson MedTech) (Figure 2B and C). One or 2 mini suture anchors are placed. One anchor is usually placed in the trapezoid and sometimes another is placed in the scaphoid (Figure 3). The anchor sutures are placed through the graft and then tied down (Figure 4A). The distal aspect of the graft is placed between the first and second metacarpal bases and anchored to the trapezoid, and the proximal end is placed between the thumb metacarpal and the scaphoid (Figure 4B and C).
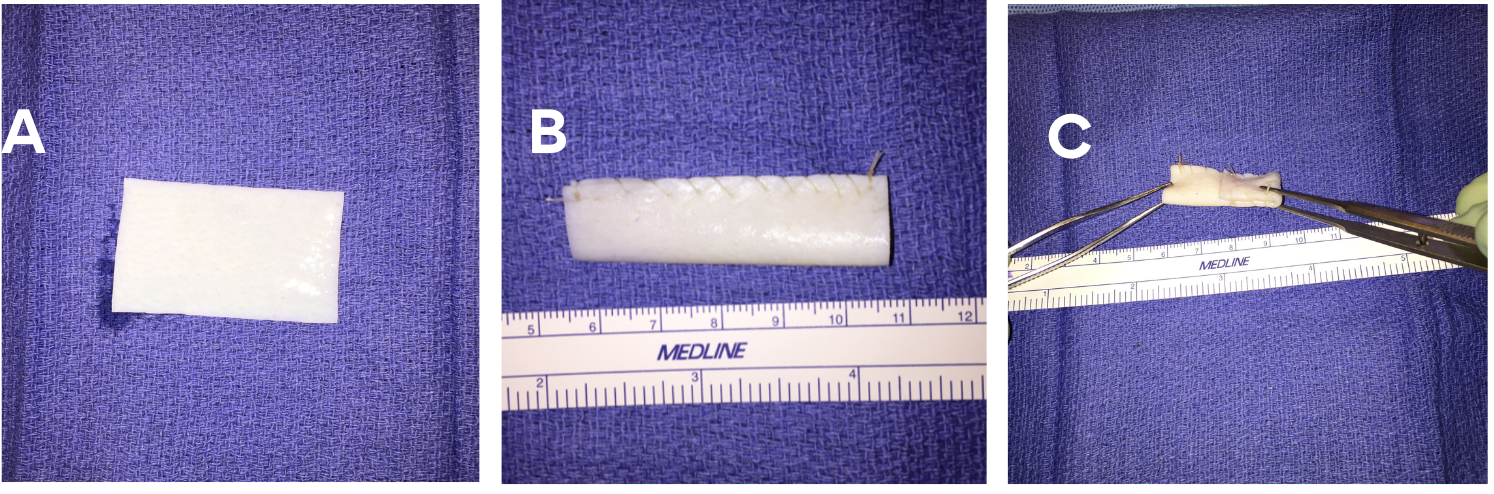
Figure 2. (A) The 2 x 4-cm Conexa raft (Tornier, Inc). (B) The Conexa graft folded longitudinally. (C) The final folded Conexa graft.
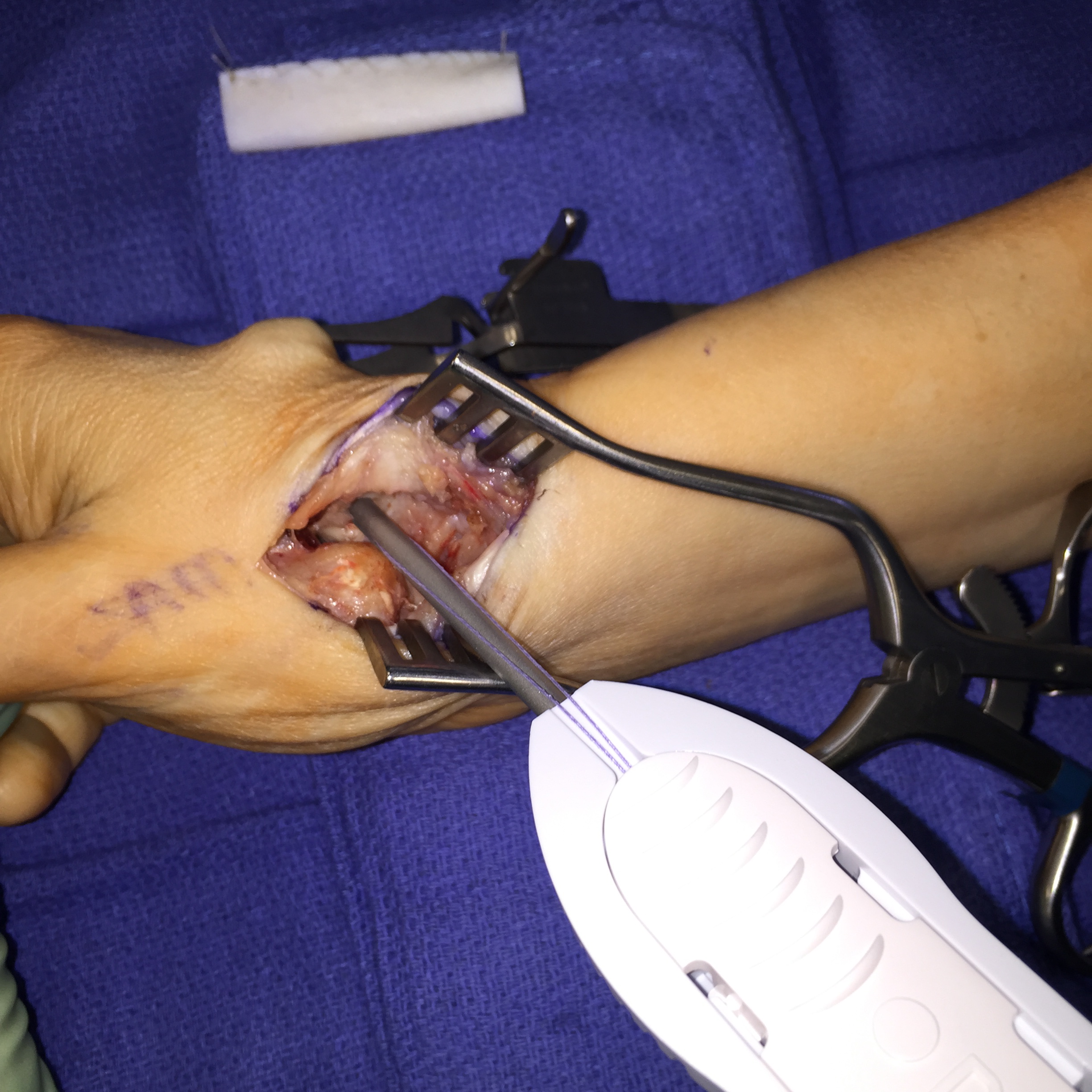
Figure 3. The suture anchor is placed in the trapezoid.
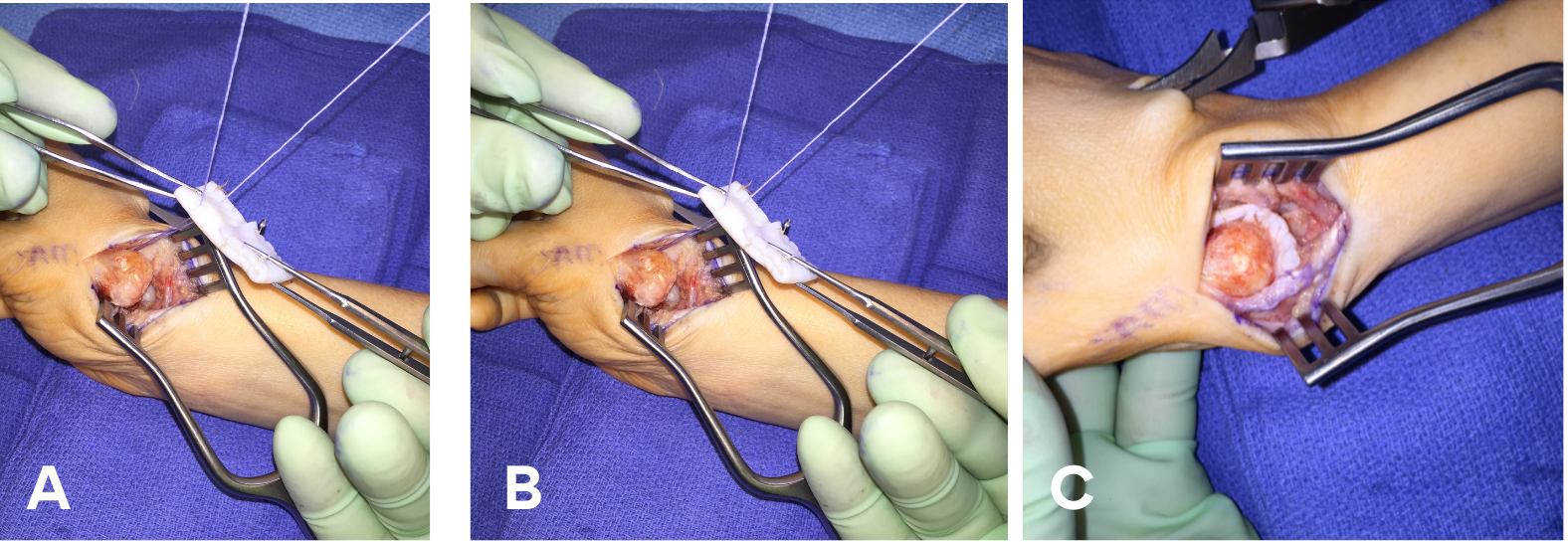
Figure 4. (A)The trapezoid anchor is sewed to the Conexa graft (Tornier, Inc). (B) The graft is positioned. (C) Final position of the Conexa graft.
Intraoperative fluoroscopic views are obtained to ensure adequate positioning of the thumb metacarpal as well as appropriate spacing between the first and second metacarpals. Layered closure is performed after irrigation, and the thumb is placed into a postoperative dressing and thumb spica splint. In this thumb spica splint, the wrist is neutral, and the fingers and thumb interphalangeal joints are free. Patients are advised to elevate and work on finger range of motion (ROM). At the 1-week postoperative visit, the dressing is removed, and patients are converted to a thumb spica thermoplastic splint. They are encouraged to remove the splint every 2 to 4 hours to engage in wrist ROM and gentle active thumb ROM with circumduction and thumb tip to fingers. At postoperative week 8, patients can convert to a soft splint during the day but are still advised to wear the thermoplastic splint overnight. Patients can now work on gentle passive ROM without resistance. Finally, at postoperative week 12, patients are encouraged to use a soft splint in public and begin using putty for hand and thumb strengthening. Patients are generally seen a final time 1 year postoperative.
Methods and Materials
Following institutional review board approval, a retrospective review of all patients treated with a porcine dermal graft for failed TMA by a single surgeon at a single institution was performed. Data collected included the primary procedure performed, time from primary procedure to revision, grip strength, key pinch strength, Visual Analog Score (VAS), ROM, time to return to work, Kapandji Score, radiographs, and any complications.
Patients were included in the study if they were (1) skeletally mature, (2) had undergone only 1 previous surgery for trapeziometacarpal arthritis, and (3) had participated in at least 12 weeks of clinical and radiographic follow-up. Patients were excluded if they were (1) skeletally immature, (2) underwent revision TMA without the use of Conexa, and (3) did not meet the minimum follow-up requirements.
Three hundred fifty-five thumb TMA procedures were performed from 2005 to 2015. Of these, 9 (2.5%) were revision procedures. Seven of the 9 revisions were performed with xenograft interposition and 2 with flexor carpi radialis tendon interposition. Five males and 2 females with a mean age of 57 years (range, 48-65 years) were included for final data evaluation. The dominant extremity was involved in 4 of the 7 patients.
Original procedures included flexor carpi radialis ligament reconstruction tendon interposition (3 patients), abductor pollicis longus suspensionplasty (3 patients), and TMA titanium joint arthroplasty (1 patient). Indications for the revision procedure included subsidence of the metacarpal in a patient with recurrent pain, weakness, and instability following a previous primary TMA for thumb basilar joint arthritis.
Results
Clinical and radiographic data are shown in detail in the Table. The mean follow-up of the patients was 84 weeks (range, 15-209 weeks). The mean time from primary procedure to revision surgery was 120 weeks (range, 14-520 weeks). The mean thumb interphalangeal joint ROM was 1.7 degrees of hyperextension to 63 degrees of flexion, and the mean metacarpalphalangeal joint ROM was 8 degrees of hyperextension to 48 degrees of flexion. The mean VAS pain score on final follow-up was 2.3 out of 10, and all patients reported a notable improvement in their symptoms. The mean Kapandji Score was 8, with most patients able to oppose the operated thumb to the proximal interphalangeal joint of the small finger. The mean grip strength was 20 kg in the operated hand and 27 kg in the unaffected hand. The mean key pinch strength was 5 kg in the operated hand and 7 kg in the unaffected hand. The mean time to return to work was 12 weeks (range, 3-23 weeks). Final radiographs of the involved thumb showed a change in the first to second metacarpal space from 1.6 to 3.3 mm and a change in the thumb metacarpal-scaphoid space from 3.0 to 5.2 mm. There were no complications or immunological reactions encountered in any patient by the final follow-up.

1o = primary procedure; 1-2 MC = first-second metacarpal space; APL = abductor pollicis longus; CMC = carpometacarpal; FCR = flexor carpi radialis; F/U = follow-up in weeks; IP = interphalangeal; Kap. = Kapandji Score; LRTI = ligament reconstruction tendon interposition; MS = metacarpal scaphoid space; ROM = range of motion: RTW = return to work in weeks; TTR = time to revision in weeks; VAS = Visual Analog Score.
Discussion
Most primary procedures for trapeziometacarpal arthroplasty have been shown to have good results, with the main goal being pain relief.18,19 There are some cases, however, that continue to have pain and problems with thumb function following surgery. Failures have been related to the type of original procedure, thumb metacarpal subsidence, and impingement between the thumb and index metacarpals as well as between the thumb metacarpal and the scaphoid. Failed trapeziometacarpal arthoplasty for thumb basilar joint arthritis presents a difficult situation for the hand surgeon. Currently, there are no universally accepted surgical techniques for revision, and each case is revised based on the original procedure and current etiology of symptoms. This study aimed to describe a novel revision surgical technique and evaluate the clinical and radiographic outcomes of patients.
Most of the current hand literature describes revisions for failed trapeziometacarpal arthroplasty from silicone implants.10 A systematic review by Ganhewa et al showed that soft tissue arthroplasty procedures had less revision rates compared with implant arthroplasty.20 The need for revision implant arthroplasty has been demonstrated to be from loosening, dislocation, and persistent pain.20 Outcomes of revision TMA arthroplasty have been good in most cases, no matter the original procedure performed.21,22 It is our belief that the etiology of the continued symptoms or recurrence of symptoms after primary TMA is primarily from impingement between the thumb and index metacarpals as well as subsidence and impingement pain between the thumb metacarpal and the scaphoid. Studies have shown that this is a large contributing factor to failure.23,24 A common technique for primary and revision TMA is suspensionplasty using implants with or without tendon autograft or transfer. These usually do well; however, impingement can be an issue if this construct is overtightened, resulting in minimal space between the first and second metacarpals. This is compounded if there are existing osteophytes that have not been addressed. Placing a dermal graft between the bones can mitigate these issues.
Kokkalis et al performed a retrospective evaluation of a human acellular dermal allograft (GraftJacket; Stryker) as an interpositional material in 82 thumbs with trapeziometacarpal osteoarthritis. With a mean follow-up of 30 months, they found 80 of the thumbs to have pain relief and 66 that could oppose to the base of the small finger. Grip and key pinch strength improved by 16% and 19%, respectively. There were no signs of foreign body reaction to the allograft tissue reported.4 They also described their primary surgical technique using this human dermal graft.25 More recent studies have investigated outcomes using human dermal allograft for primary procedures, both open and arthroscopic.26,27
The current study describes a revision technique using porcine dermal graft without ligament reconstruction and tendon interposition. This technique does not create a hole within the metacarpals. This porcine graft is rehydrated within 2 minutes vs 10 to 15 minutes for the GraftJacket, saving on operating room time. Human aceullar dermal matrix has been studied for proximal row carpectomy with good outcomes, and this technique for folding the graft and sewing together along with using anchors with suture through the graft is similar to these studies.28,29
Belcher et al published on the use of a porcine dermal collagen xenograft in a randomized trial in 26 patients comparing trapeziectomy alone and interposition with xenograft as a primary procedure. Immunogenic reactions occurred in 6 of the 13 patients with the porcine dermal collagen xenograft, and 3 of these were removed. They concluded that trapeziectomy alone was better.15 Our results contrast with this, as none of our 7 patients experienced an immunogenic reaction and no graft needed to be removed at the mean follow-up of over a year. This could be due to a difference in the porcine graft used. To our knowledge, this is the first study evaluating the use of porcine dermal matrix for revision trapeziometacarpal arthritis.
The current study shows encouraging results with the use of a porcine dermal matrix for interposition for revision of failed TMA. This technique is primarily a distraction arthroplasty with the use of xenograft to assist in positioning of the thumb metacarpal to remedy the offending impingement. Conexa is designed for cell ingrowth and incorporates fully approximately 6 months from the time of surgery. This may allow for a more substantial hematoma and scar formation for continued protection against impingement. We did not perform a suspensionplasty alongside this interposition; however, this technique has also been shown to do well and is an option. This series of patients shows good outcomes without adjunct of suture or tendon suspensionplasty; in addition, the extra cost of implants and the need for tendon graft harvest or transfer was avoided. This technique is easily reproducible and addresses impingement between the thumb and index metacarpal as well as between the thumb metacarpal and scaphoid.
Limitations
The current study was limited by its retrospective design, lack of comparison group, and preoperative clinical data. Another potential limitation of the study is the small number of patients included and relatively short period of follow-up. The small cohort of patients is due to revision TMA representing a relatively small percentage of hand surgery practice, and the percentage of revisions was consistent with what is seen clinically and in the literature. The length of follow-up is consistent with other studies and reflects the standard clinical follow-up for trapeziometacarpal arthroplasty surgery. Future studies with a comparison group and longer follow-up will be necessary to further understand the full benefits of this surgical technique in comparison to others. This study looks at 1 particular porcine graft; however, outcomes with other xenografts and human dermal graft may likely be similar.
Conclusions
The results of this study indicate that the use of a porcine dermal matrix for interposition to remove impingement provides benefits to patients who suffer from continued pain and difficulty in use of the thumb after their primary TMA. This is a relatively simple technique using a type of graft that is readily available and has been shown to be safe in human application
Acknowledgments
Authors: Michael C. Doarn, MD1; Mariel McLaughlin McArthur, MD2; John J. Fernandez, MD3
Affiliations: 1Florida Orthopaedic Institute, Tampa, Florida; 2Department of Plastic Surgery, University of South Florida, Tampa, Florida; 3Midwest Orthopaedics at Rush, Rush University Medical Center, Chicago, Illinois.
Correspondence: Michael C. Doarn, MD, 5901 E Fowler Ave, Suite 100, Temple Terrace, FL 33617, USA. Email: Mdoarn7@gmail.com
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
- Trumble TE, Rafijah G, Gilbert M, Allan CH, North E, McCallister WV. Thumb trapeziometacarpal joint arthritis: partial trapeziectomy with ligament reconstruction and interposition costochondral allograft. J Hand Surg Am. 2000;25(1):61-76. doi:10.1053/jhsu.2000.jhsu025a0061
- Shapiro PS, Diao E, Givens LM. Meniscal allograft arthroplasty for the treatment of trapeziometacarpal arthritis of the thumb. Hand (N Y). 2015;10(3):407-416. doi:10.1007/s11552-014-9737-4
- Spaans AJ, van Heeswijk EJ, Arnold DE, Beumer A. Foreign body reaction associated with polyethylene mesh interposition used for treatment of trapeziometacarpal osteoarthritis: report of 8 cases. J Hand Surg Am. 2014;39(10):2016-2019. doi:10.1016/j.jhsa.2014.07.038
- Kokkalis ZT, Zanaros G, Weiser RW, Sotereanos DG. Trapezium resection with suspension and interposition arthroplasty using acellular dermal allograft for thumb carpometacarpal arthritis. J Hand Surg Am. 2009;34(6):1029-1036. doi:10.1016/j.jhsa.2009.03.001
- Gillis J, Calder K, Williams J. Review of thumb carpometacarpal arthritis classification, treatment and outcomes. Can J Plast Surg. 2011;19(4):134-138. doi:10.1177/229255031101900409
- Greenberg JA, Mosher JF Jr, Fatti JF. X-ray changes after expanded polytetrafluoroethylene (Gore-Tex) interpositional arthroplasty. J Hand Surg Am. 1997;22(4):658-663. doi:10.1016/S0363-5023(97)80125-6
- Cooney WP 3rd, Leddy TP, Larson DR. Revision of thumb trapeziometacarpal arthroplasty. J Hand Surg Am. 2006;31(2):219-227. doi:10.1016/j.jhsa.2005.10.018
- Vermeulen GM, Slijper H, Feitz R, Hovius SE, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg Am. 2011;36(1):157-169. doi:10.1016/j.jhsa.2010.10.028
- Naidu SH, Kulkarni N, Saunders M. Titanium basal joint arthroplasty: a finite element analysis and clinical study. J Hand Surg Am. 2006;31(5):760-765. doi:10.1016/j.jhsa.2005.12.022
- Kaszap B, Daecke W, Jung M. Outcome comparison of primary trapeziectomy versus secondary trapeziectomy following failed total trapeziometacarpal joint replacement. J Hand Surg Am. 2013;38(5):863-871.e3. doi:10.1016/j.jhsa.2013.01.030
- Braun RM, Rechnic M, Shah KN. Salvage reconstruction of failed interposition arthroplasty at the base of the thumb. Tech Hand Up Extrem Surg. 2012;16(4):230-235. doi:10.1097/BTH.0b013e31826cf1bb
- Birman MV, Strauch RJ. Update on nonautogenous interposition arthroplasty for thumb basilar joint arthritis. J Hand Surg Am. 2011;36(12):2056-2059. doi:10.1016/j.jhsa.2011.09.041
- Kozlow JH, Beil RJ, Chung KC. Repair of symptomatic forearm hernias using acellular dermal matrix--two case reports. J Hand Surg Am. 2010;35(12):2053-2056. doi:10.1016/j.jhsa.2010.07.035
- Papatheodorou LK, Williams BG, Sotereanos DG. Preliminary results of recurrent cubital tunnel syndrome treated with neurolysis and porcine extracellular matrix nerve wrap. J Hand Surg Am. 2015;40(5):987-992. doi:10.1016/j.jhsa.2015.02.031
- Belcher HJ, Zic R. Adverse effect of porcine collagen interposition after trapeziectomy: a comparative study. J Hand Surg Br. 2001;26(2):159-164. doi:10.1054/jhsb.2001.0554
- Xu H, Sandor M, Qi S, et al. Implantation of a porcine acellular dermal graft in a primate model of rotator cuff repair. J Shoulder Elbow Surg. 2012;21(5):580-588. doi:10.1016/j.jse.2011.03.014
- Shea KP, Obopilwe E, Sperling JW, Iannotti JP. A biomechanical analysis of gap formation and failure mechanics of a xenograft-reinforced rotator cuff repair in a cadaveric model. J Shoulder Elbow Surg. 2012;21(8):1072-1079. doi:10.1016/j.jse.2011.07.024
- Eaton RG, Glickel SZ, Littler JW. Tendon interposition arthroplasty for degenerative arthritis of the trapeziometacarpal joint of the thumb. J Hand Surg Am. 1985;10(5):645-654. doi:10.1016/s0363-5023(85)80201-x
- Wolf JM, Delaronde S. Current trends in nonoperative and operative treatment of trapeziometacarpal osteoarthritis: a survey of US hand surgeons. J Hand Surg Am. 2012;37(1):77-82. doi:10.1016/j.jhsa.2011.10.010
- Ganhewa AD, Wu R, Chae MP, et al. Failure rates of base of thumb arthritis surgery: a systematic review. J Hand Surg Am. 2019;44(9):728-741.e10. doi:10.1016/j.jhsa.2019.05.003
- Renfree KJ, Dell PC. Functional outcome following salvage of failed trapeziometacarpal joint arthroplasty. J Hand Surg Br. 2002;27(1):96-100. doi:10.1054/jhsb.2001.0648
- Conolly WB, Rath S. Revision procedures for complications of surgery for osteoarthritis of the carpometacarpal joint of the thumb. J Hand Surg Br. 1993;18(4):533-539. doi:10.1016/0266-7681(93)90166-d
- Roman PB, Linnell JD, Moore JB. Trapeziectomy arthroplasty with suture suspension: short- to medium-term outcomes from a single-surgeon experience. J Hand Surg Am. 2016;41(1):34-39.e1. doi:10.1016/j.jhsa.2015.10.010
- Yang SS, Weiland AJ. First metacarpal subsidence during pinch after ligament reconstruction and tendon interposition basal joint arthroplasty of the thumb. J Hand Surg Am. 1998;23(5):879-883. doi:10.1016/S0363-5023(98)80167-6
- Kokkalis ZT, Zanaros G, Sotereanos DG. Ligament reconstruction with tendon interposition using an acellular dermal allograft for thumb carpometacarpal arthritis. Tech Hand Up Extrem Surg. 2009;13(1):41-46. doi:10.1097/BTH.0b013e31818be857
- Logli AL, Twu J, Bear BJ, Lindquist JR, Schoenfeldt TL, Korcek KJ. Arthroscopic partial trapeziectomy with soft tissue interposition for symptomatic trapeziometacarpal arthritis: 6-month and 5-year minimum follow-up. J Hand Surg Am. 2018;43(4):384.e1-384.e7. doi:10.1016/j.jhsa.2017.10.016
- Marks M, Hensler S, Wehrli M, Scheibler AG, Schindele S, Herren DB. Trapeziectomy with suspension-interposition arthroplasty for thumb carpometacarpal osteoarthritis: a randomized controlled trial comparing the use of allograft versus flexor carpi radialis tendon. J Hand Surg Am. 2017;42(12):978-986. doi:10.1016/j.jhsa.2017.07.023
- Rabinovich RV, Lee SJ. Proximal row carpectomy using decellularized dermal allograft. J Hand Surg Am. 2018;43(4):392.e1-392.e9. doi:10.1016/j.jhsa.2018.01.012
- Lee SJ, Rabinovich RV, Kim A. Proximal row carpectomy using decellularized dermal allograft: preliminary results. J Wrist Surg. 2021;10(2):116-122. doi:10.1055/s-0040-1718912