Double Recurrence of Lipoma Following Liposuction: Highlighting the Potential for Cannular Seeding
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- What are the characteristic clinical features of subcutaneous lipomas of the trunk, and what is the differential diagnosis of a superficial back mass?
- What are the available surgical techniques for lipoma removal, and what are the considerations when choosing between liposuction and open excision?
- What are the potential complications of lipoma management, and what clinical features raise concern for malignant transformation into liposarcoma?
- How often do lipomas recur after treatment, and what influences the likelihood of recurrence?
Case Description
A 24-year-old healthy woman presented with a recurrent lipomatous mass on her upper back following 2 prior attempts at liposuction excision by an outside plastic surgeon. The patient reported that the current recurrence was larger than the previous one, and she now desired definitive surgical management. Magnetic resonance imaging (MRI) was obtained following initial evaluation and demonstrated a subcutaneous lipoma measuring 8.9 x 10.7 cm, located at the mid-thoracic level just right of the paraspinal region (Figure 1). The patient was taken to the operating room for wide local excision. Following excision, the wound cavity was palpated to ensure complete removal. Palpation revealed an additional segment of lipomatous tissue branching from the primary tumor. The tissue was excised and the cavity was once again palpated, which revealed another similar branch of lipomatous tissue. This sequence was repeated multiple times, ultimately revealing 5 additional discrete areas of mature adipose tissue with surrounding fibrosis adjacent to the primary mass, suggestive of peripheral seeding from prior liposuction attempts (Figure 2). Because these branches were adjoining and congruent, they were not distinguishable on preoperative MRI and, thus, the lipomas were interpreted as a single mass. All involved areas were submitted for histopathologic analysis. Final pathology confirmed mature adipose tissue without atypia and negative MDM2 staining by immunohistochemistry, consistent with a benign lipoma. Importantly, there has been no evidence of recurrence at 12 months postoperative (Figure 3).

Figure 1. Preoperative photograph of the lipomatous mass located in the patient's right upper parathoracic region prior to wide local excision.
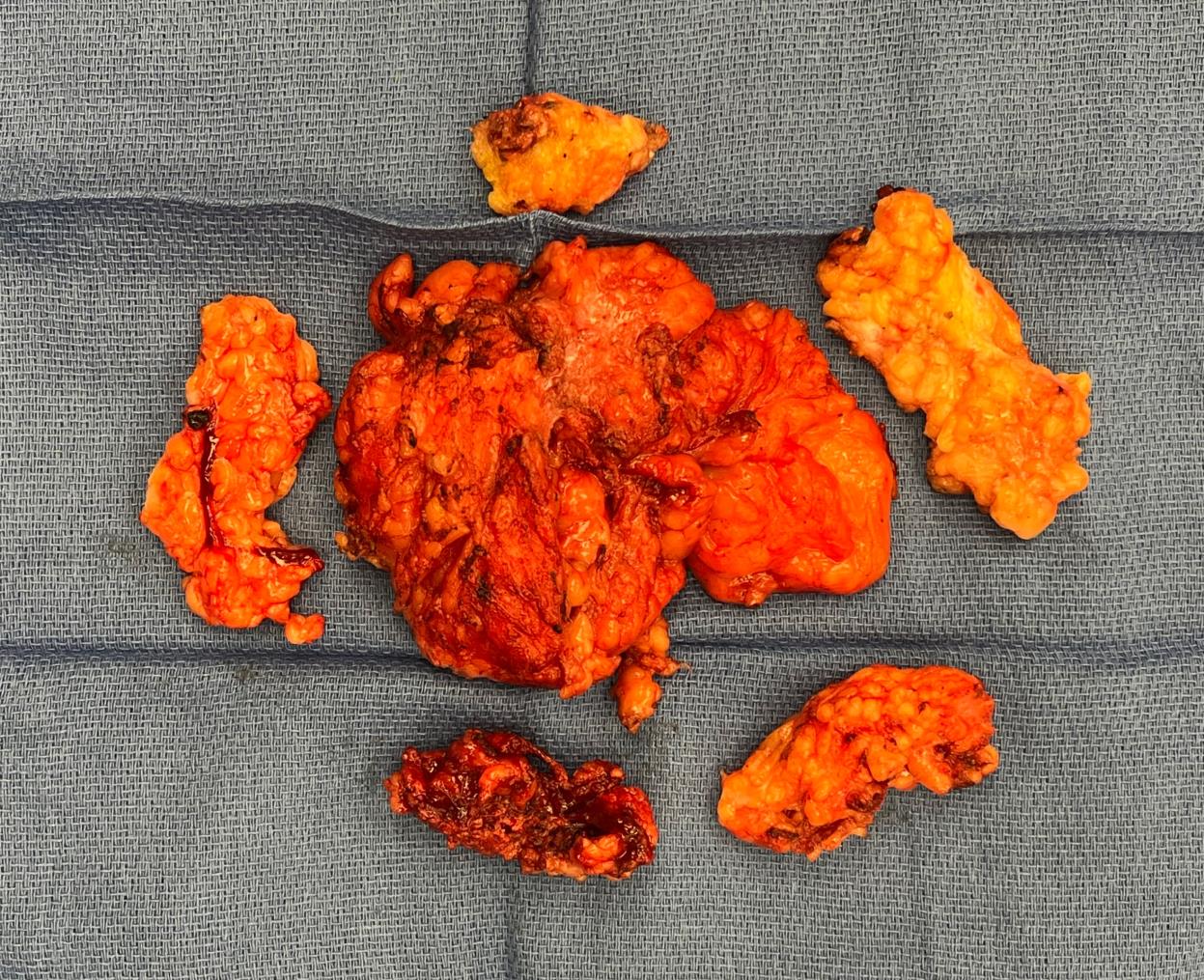
Figure 2. Intraoperative photograph of the multiple discrete lipomatous specimens immediately following excision and prior to submission for histopathologic evaluation.
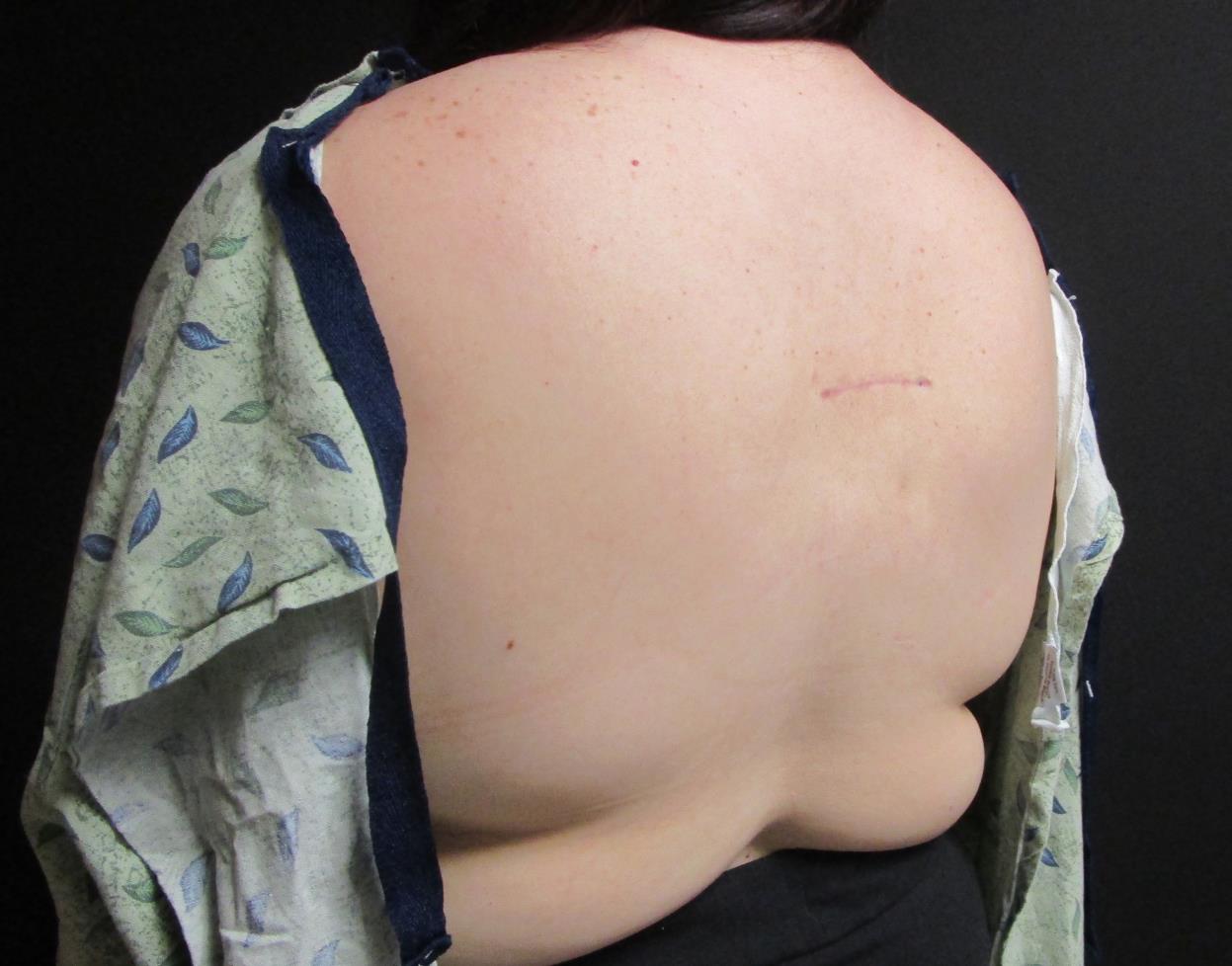
Figure 3. Longitudinal clinical photograph at the 12-month postoperative follow-up demonstrated no clinical evidence of recurrence.
This case presentation uniquely illustrates a rare presentation of iatrogenic lipoma recurrence likely due to peripheral seeding from prior liposuction, prompting critical reevaluation of surgical technique, recurrence patterns, and diagnostic vigilance in distinguishing benign from malignant soft tissue tumors.
Q1: What are the characteristic clinical features of subcutaneous lipomas of the trunk, and what is the differential diagnosis of a superficial back mass?
Lipomas are the most common benign soft tissue mesenchymal neoplasms of the human body, with a prevalence of 2.1 per 1000 people.1,2 They occur most frequently on the arm, shoulder, back, legs, forehead, and face.3 Most lipomas range from 1 to 10 cm, with lipomas greater than 10 cm classified as giant lipomas.4 The presence of multiple lipomas may be indicative of a variety of syndromes.4
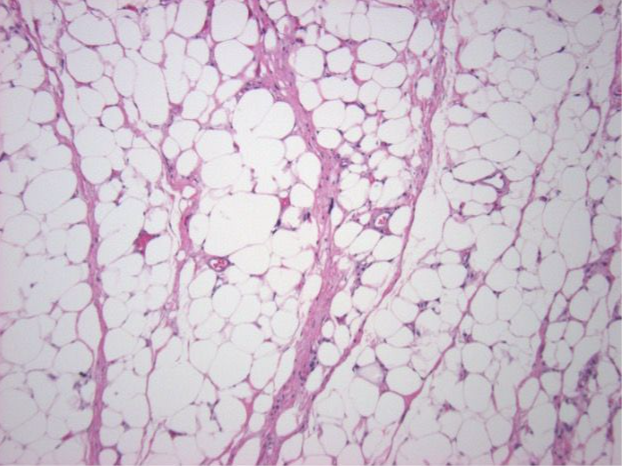
Lipomas are generally painless, subcutaneous, well-circumscribed, mobile, soft, solitary, and slow-growing masses with the absence of epidermal change.1,4 Histologically, lipomas are composed of mature, normal-appearing adipocytes with small eccentric nucleus—thus indistinguishable from adipocytes in the subcutaneous tissue.4 Histology is important in distinguishing a benign lipoma from liposarcomas, which are a malignant lipomatous neoplasm. The absence of vacuoles in irregularly shaped hyperchromatic nuclei and an increased cell size can be helpful in the differentiation between lipomas and liposarcomas.5 A differential diagnosis for a subcutaneous mass on a trunk can commonly include—but is not limited to—epidermoid cysts, hibernomas, angiolipomas, angiomyolipomas, and liposarcomas.1,4 Epidermoid cysts frequently display a central punctum on the surface and are attached or fixed to the overlying skin.4 Hibernomas are rare, benign tumors composed of brown adipose tissue, most often located in the mediastinum or the interscapular region of the back, and generally present in adults as slow-growing masses measuring between 3 and 12 centimeters.4 Angiolipomas are characteristically painful, well-defined lesions typically less than 2 centimeters in diameter, and are most commonly found on the forearms of adolescents or young adults.4 Angiomyolipomas tend to arise in acral sites and are more frequently seen in adult males.4 Liposarcomas usually manifest as deep-seated tumors with a predilection for the retroperitoneum or, classically, the thigh.
Q2: What are the available surgical techniques for lipoma removal, and what are the considerations when choosing between liposuction and open excision?
A variety of techniques exist for lipoma removal, including injection lipolysis, liposuction, and open surgical excision. Patients commonly seek treatment because of aesthetic concerns, discomfort, compressive symptoms, or oncologic anxiety.6 Liposuction for lipoma removal was first popularized by Rubinstein et al in 1985 as a less invasive alternative associated with fewer complications.7 Early proponents of liposuction emphasized its cosmetic advantages, such as reduced scarring, decreased intraoperative bleeding, contouring capability, shorter operative times, cost-effectiveness, and the ability to address multiple lesions through fewer incisions.8,9 However, its efficacy was initially met with skepticism by some.10 The decision to pursue liposuction vs open excision is largely guided by shared decision-making between the patient and surgeon. Liposuction is typically favored for well-circumscribed, suprafascial lesions—either solitary or multiple—that are moderate to large in size with a confirmed benign diagnosis.6 Given the inability to obtain a specimen with intact margins, preoperative evaluation to exclude malignancy is paramount. At minimum, fine needle aspiration and ultrasound imaging have been recommended to ensure diagnostic certainty prior to proceeding with liposuction.11
Conventional open excision is often regarded as the gold standard for lipoma removal, as it allows for complete en bloc resection and histopathologic evaluation.12 The surgical approach varies depending on the size and location of the lesion. For small, superficial lipomas, techniques such as punch excision, linear incision, or elliptical excision are commonly employed.13-16 In contrast, larger lipomas may necessitate more advanced planning to optimize exposure while minimizing incision length and visible scarring. Reported approaches for larger lesions include extended linear incisions, large elliptical excisions, Z-plasty techniques, and one-third incisions, each tailored to achieve adequate exposure and aesthetic outcomes.12,16-18
Q3: What are the potential complications of lipoma management, and what clinical features raise concern for malignant transformation into liposarcoma?
As with any surgical intervention, lipoma management carries the risk of complications, which vary depending on the chosen technique. Critics of liposuction argue that the approach limits direct visualization, fragments the specimen—complicating histopathologic evaluation—and may leave behind residual lipomatous or capsular tissue, increasing the risk of recurrence.19-21 In addition to common postoperative issues such as seroma and hematoma formation, delayed complications including contour irregularities and cutaneous depressions have also been reported.6 Notably, similar complications can occur following open excision, including seroma, hematoma, nerve injury, and residual mass due to incomplete resection.17,18
Histologically, well-differentiated liposarcoma (WDLS) is characterized by mature adipocytes interspersed with varying numbers of hyperchromatic, spindle-shaped cells and multivacuolated lipoblasts.22 Immunohistochemical analysis often reveals CDK4 positivity, present in approximately 62% of cases.22 Despite concerns about malignant transformation, true recurrence of a benign lipoma as a liposarcoma is exceedingly rare, with only isolated case reports documented in the literature.23,24 Notably, both reported cases of recurrent WDLS shared certain risk factors, including large (≥5 cm) or giant lipomas and atypical tumor locations.23 These findings underscore the importance of thorough preoperative assessment. Sonographic features such as deep location, septations, irregular borders, hyperechogenicity, vascularity, and large size should prompt further evaluation.25 In such cases, MRI is the gold standard for advanced imaging.23 Additionally, recent studies suggest that the combination of p16 immunohistochemistry with MDM2 fluorescence in situ hybridization staining enhances diagnostic accuracy in distinguishing WDLS from deep-seated benign lipomas.26
Q4: How often do lipomas recur after treatment, and what influences the likelihood of recurrence?
The recurrence rate following open lipectomy has been reported to be approximately 2%.27 Unfortunately, recurrence rates following liposuction alone are infrequently cited in the literature. When outcomes are reported, liposuction is often performed in conjunction with surgical excision, which limits applicability to cases managed with liposuction as a standalone technique. One study from 1992 noted an “unacceptably high recurrence rate” following isolated liposuction.10 Proposed reasons for recurrence after liposuction include limited visualization, incomplete removal of lipomatous or capsular tissue, deep-seated or giant lipomas, septated architecture, tissue fragmentation with possible seeding, and failure to excise the capsule—each of which may predispose to residual disease and recurrence.6,28,29 It is important to note that tissue fragmentation with potential seeding has been identified as a risk factor for recurrence.29 Additionally, the fragmentation inherent to liposuction may compromise the integrity of the specimen, limiting the ability to perform accurate histopathologic evaluation—particularly in cases where there is clinical concern for malignancy.6
In conclusion, we present the unique case of a 24-year-old woman with a recurrent truncal lipoma following 2 unsuccessful attempts at removal via liposuction alone. Definitive management was ultimately achieved through wide local excision, with no evidence of recurrence at 12 months postoperative. This case is notable given the paucity of literature reporting recurrence rates following liposuction alone and, to our knowledge, there are no previously documented cases of multiple recurrences after isolated liposuction. Intraoperatively, 5 discrete lipomatous masses were identified, highlighting a potential complication of liposuction—namely, tissue fragmentation with possible seeding—an outcome that has been theorized but rarely demonstrated in the literature. These findings suggest that the recurrence pattern in this patient may have resulted from iatrogenic dissemination. Additionally, this case underscores the importance of comprehensive preoperative evaluation, particularly when liposuction is considered. Inadequate oncologic control due to failure to excise the capsule, coupled with an inaccurate benign diagnosis, could theoretically permit malignant transformation or residual disease. Ultimately, this case emphasizes the need for careful selection of treatment modality and reinforces the real risk of recurrence when liposuction is used as the sole method of lipoma removal.
Acknowledgments
Authors: Ryan A. Cantrell, BS1; Colton H. Connor, BS1; Quinton L. Carr, BA1; Bradon J. Wilhelmi, MD2
Affiliations: 1University of Louisville School of Medicine, Louisville, Kentucky; 2Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky
Correspondence: Bradon J. Wilhelmi, MD, Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Louisville, 550 South Jackson Street, ACB 2nd Floor, Louisville, KY 40202, USA. Email: bradon.wilhelmi@louisville.edu
Ethics: The patient illustrated in this document has been provided informed consent on the use of their images and granted the use of their images for scientific publications.
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Derin AT YN. Lipomas: Review and Evaluation of the Literature. Clinics in Surgery. 2017;2:1615.
2. K. L. Kumari VPVSSB, S. V. Kumar. Giant Intermuscular Lipoma of Neck and Chest: A Case Report with Review of Literature. International Journal of Research in Medical Sciences. 2015;3(6):1521-1523. doi:10.18203/2320-6012.ijrms20150198
3. R. Gaur RLS, S. Rai. Giant Lipoma in Front of the Neck Presenting as Thyroid Neoplasm: A Rare Case. International Journal of Medical Science Research and Practice. 2015;2(1):41-43.
4. Logan Kolb SNSY, Muhammad Atif Ameer, Juan A. Rosario-Collazo. StatPearls. Lipoma. StatPearls Publishing; 2023.
5. Forcucci JA, Sugianto, J. Z., Wolff, D. J., Maize, J. C. Sr., & Ralston, J. S. Low-Fat Pseudoangiomatous Spindle Cell Lipoma: A Rare Variant With Loss of 13q14 Region. The American Journal of Dermatopathology. 2015;37(12):920-923. doi:10.1097/DAD.0000000000000286
6. Peev I, Spasevska L, Mirchevska E, Tudzarova-Gjorgova S. Liposuction Assisted Lipoma Removal - Option or Alternative? Open Access Maced J Med Sci. Oct 15 2017;5(6):766-770. doi:10.3889/oamjms.2017.186
7. Rubenstein R, Roenigk HH, Jr., Garden JM, Goldberg NS, Pinski JB. Liposuction for lipomas. J Dermatol Surg Oncol. Nov 1985;11(11):1070-4. doi:10.1111/j.1524-4725.1985.tb01395.x
8. Coleman WP, 3rd. Noncosmetic applications of liposuction. J Dermatol Surg Oncol. Oct 1988;14(10):1085-90. doi:10.1111/j.1524-4725.1988.tb03465.x
9. Spinowitz AL. Liposuction surgery: an effective alternative for treatment of lipomas. Plast Reconstr Surg. Sep 1990;86(3):606.
10. Raemdonck D, De Mey A, Goldschmidt D. [The treatment of giant lipomas]. Acta Chir Belg. Jul-Aug 1992;92(4):213-6. Le traitement des lipomes geants.
11. Choi CW, Kim BJ, Moon SE, Youn SW, Park KC, Huh CH. Treatment of lipomas assisted with tumescent liposuction. J Eur Acad Dermatol Venereol. Feb 2007;21(2):243-6. doi:10.1111/j.1468-3083.2006.02037.x
12. M. B. A review of techniques and procedures for lipoma treatment. Clinics in Dermatology. 2015;3(4):105–112. doi:10.11138/cderm/2015.3.4.105.
13. Myhre-Jensen O. A consecutive 7-year series of 1331 benign soft tissue tumours. Clinicopathologic data. Comparison with sarcomas. Acta Orthop Scand. Jun 1981;52(3):287-93. doi:10.3109/17453678109050105
14. Christenson L, Patterson J, Davis D. Surgical pearl: use of the cutaneous punch for the removal of lipomas. J Am Acad Dermatol. Apr 2000;42(4):675-6.
15. Ronan SJ, Broderick T. Minimally invasive approach to familial multiple lipomatosis. Plast Reconstr Surg. Sep 2000;106(4):878-80. doi:10.1097/00006534-200009040-00021
16. Cosulich MT, Molenda MA, Mostow E, Bhatia AC, Brodell RT. Minimal incision extraction of lipomas. JAMA Dermatol. Dec 2014;150(12):1360-1. doi:10.1001/jamadermatol.2014.3234
17. Park JK, Kim J, Kim JH, Eun S. Minimal One-Third Incision and Four-Step (MOTIF) Excision Method for Lipoma. Biomed Res Int. 2021;2021:4331250. doi:10.1155/2021/4331250
18. Won JH, Hur K, Ohn J, Mun JH. Surgical management of lipomas: Proposal of the Z-incision design and surgical algorithm based on tumor size. Dermatol Ther. Jan 2020;33(1):e13151. doi:10.1111/dth.13151
19. Hallock GG. Endoscope-assisted suction extraction of lipomas. Ann Plast Surg. Jan 1995;34(1):32-4. doi:10.1097/00000637-199501000-00007
20. Silistreli OK DE, Ulusal BG, Oztan Y, Görgü M. What should be the treatment modality in giant cutaneous lipomas? Review of the literature and report of 4 cases. British Journal of Plastic Surgery. 2005;58(3):394-398.
21. Ilhan H, Tokar B. Liposuction of a pediatric giant superficial lipoma. J Pediatr Surg. May 2002;37(5):796-8. doi:10.1053/jpsu.2002.32291
22. de Bree E, Karatzanis A, Hunt JL, et al. Lipomatous tumours of the head and neck: a spectrum of biological behaviour. Eur Arch Otorhinolaryngol. May 2015;272(5):1061-77. doi:10.1007/s00405-014-3065-8
23. Lee YJ, Cha WJ, Kim Y, Oh DY. The recurrence of well-differentiated liposarcoma from benign giant intramuscular lipoma: A case (CARE-compliant) report. Medicine (Baltimore). Feb 12 2021;100(6):e24711. doi:10.1097/MD.0000000000024711
24. Widodo W LW, Aprilya D. Well-differentiated liposarcoma disguised as a recurrent lipoma of the forearm flexor compartment: A case report. International Journal of Surgery Case Reports. 2020;72:91–95. doi:10.1016/j.ijscr.2020.05.063
25. Shimamori N, Kishino T, Okabe N, et al. Discrimination of well-differentiated liposarcoma from benign lipoma on sonography: an uncontrolled retrospective study. J Med Ultrason (2001). Oct 2020;47(4):617-623. doi:10.1007/s10396-020-01051-5
26. Kammerer-Jacquet SF, Thierry S, Cabillic F, et al. Differential diagnosis of atypical lipomatous tumor/well-differentiated liposarcoma and dedifferentiated liposarcoma: utility of p16 in combination with MDM2 and CDK4 immunohistochemistry. Hum Pathol. Jan 2017;59:34-40. doi:10.1016/j.humpath.2016.08.009
27. Dalal KM, Antonescu CR, Singer S. Diagnosis and management of lipomatous tumors. J Surg Oncol. Mar 15 2008;97(4):298-313. doi:10.1002/jso.20975
28. Copeland-Halperin LR, Pimpinella V, Copeland M. Combined liposuction and excision of lipomas: long-term evaluation of a large sample of patients. Plast Surg Int. 2015;2015:625396. doi:10.1155/2015/625396
29. Wilhelmi BJ BS, Mancoll JS, Phillips LG. Another indication for liposuction: small facial lipomas. Plastic and Reconstructive Surgery. 1999;103(7):1864-1867. doi:10.1097/00006534-199906000-00008.