The Impact of Eyebrow and Eyelash Loss
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of The Dermatologist or HMP Global, their employees, and affiliates.

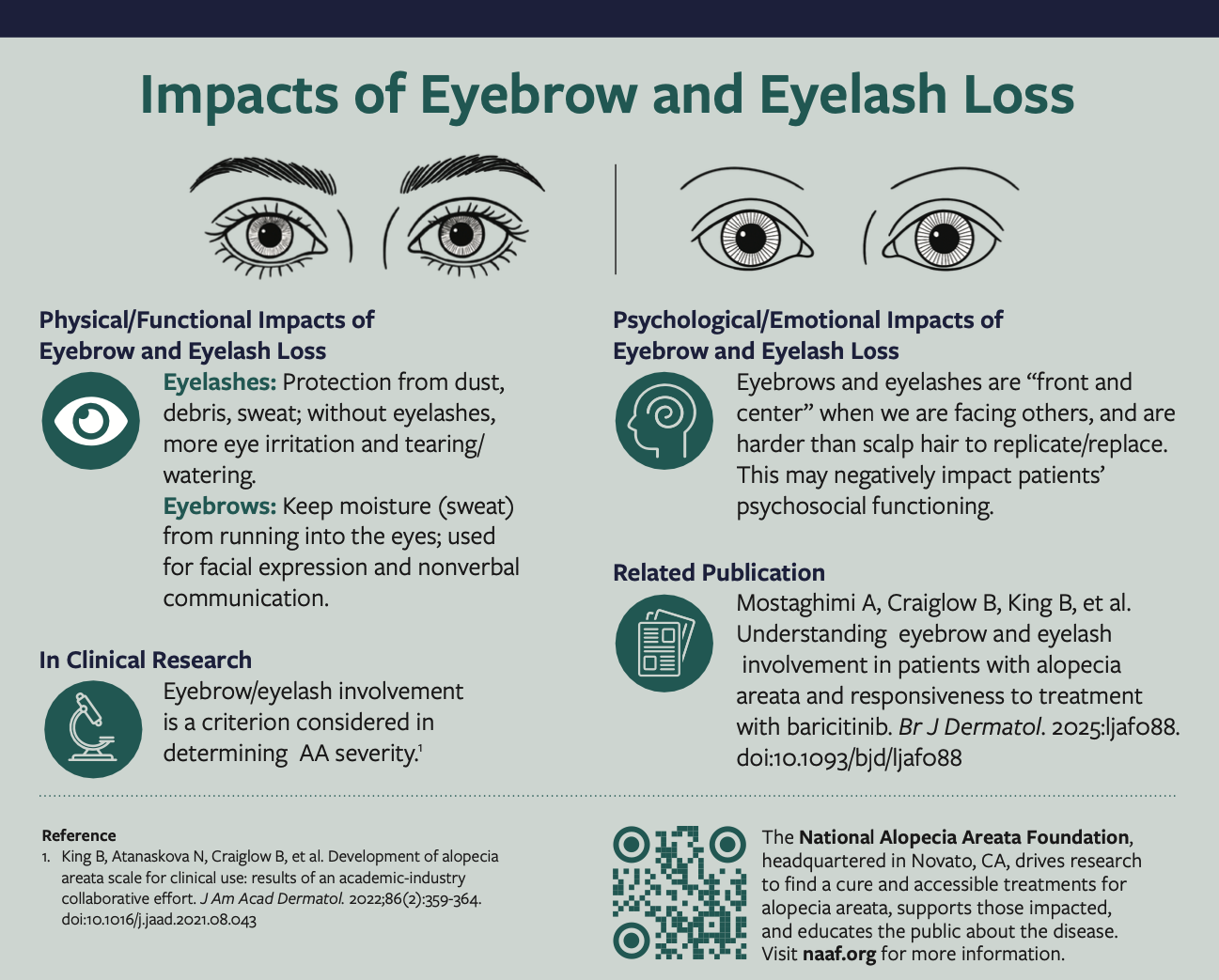
Eyebrow and eyelash loss in patients with alopecia areata (AA) can have profound psychological, emotional, and functional impacts, yet it has historically been overlooked. In an insightful conversation with Dr Melissa Piliang, we explore how the loss of these facial features affects patients’ quality of life, advancements in treatment options, and how new clinical trials are offering hope for patients seeking eyebrow and eyelash restoration.
The Dermatologist: Can you discuss the psychological and emotional impact of eyebrow and eyelash loss in patients with AA, and how does this differ from scalp hair loss?
Dr Piliang: Eyebrows and eyelashes are important because they are front and center when we meet somebody, and in contrast to scalp hair, they are very hard to replicate or replace. Even if you get tattooed eyebrows or draw them in, they are still flat rather than three-dimensional. Patients can get very good wigs that can effectively cover their scalp, but it is much harder to cover eyebrows and eyelashes. They are also functionally important. Eyebrows serve as a barrier to protect the eye, keeping sweat and anything that you put on your scalp or forehead from running into your eyes. If you do not have eyebrows and you put on sunscreen and then go outside and get sweaty, all the sunscreen and everything that is on your forehead runs into your eyes and burns. It is the same thing with eyelashes. My patients who do not have eyelashes tell me that they get more grit and dirt in their eyes. They get more eye irritation, tearing, and watering. They even feel like if they roll over in the night, it irritates their eye because they do not have eyelashes there to protect them. We really must think about not just the psychosocial impact, but also the functional impact and understand that treating eyebrow and eyelash loss is worthwhile.
The Dermatologist: Why has the loss of eyebrows and eyelashes in AA been historically underappreciated, and what changes have you seen in its recognition in recent years?
Dr Piliang: I think some of it comes from just not having good treatments for AA for a long time. We had very limited treatment that we could do. For example, my office does injections for eyebrows, but it is much harder and more painful for patients’ eyelashes. So, our patients would find ways to cover cosmetically as best as they could. But now we have good, safe options both topically and orally that can help grow eyebrows and eyelashes. It is now part of the conversations we have. I have patients who go on a Janus kinase (JAK) inhibitor, and they only grow back eyebrow and eyelash hair, but they are still very happy because their eyebrows and eyelashes are immensely important to them.

The Dermatologist: How are clinical trials addressing the issue of eyebrow and eyelash loss in AA, and are there specific outcomes being measured in these areas?
Dr Piliang: The clinical trials for JAK inhibitors have really helped with the increased emphasis on eyebrow and eyelash involvement in AA. Eyebrow and eyelash regrowth was one of the monitored outcomes, and a 4-point scale was used to determine success: full eyebrows or eyelashes; minimal patchy loss; significant loss, but still a few eyebrow/eyelash hairs; and complete loss. To be considered responders in the trials, patients had to go from either complete loss or near complete loss and move up 2 points. So, if they had complete loss, they either had to have near complete regrowth or full eyebrows and if they had minimal eyebrows or eyelashes, they had to go to complete regrowth.
The Dermatologist: Do you foresee any changes in future clinical trial designs to better capture the impact of eyebrow and eyelash loss in AA?
Dr Piliang: I expect that clinical trials will continue to include eyebrows and eyelashes as an outcome. It would be great if we could capture the percent of regrowth in a more specific way using photos and maybe artificial intelligence in clinical trials moving forward.
The Dermatologist: You mentioned JAK inhibitors, what role do they play in regrowing eyebrows and eyelashes and is there evidence supporting their efficacy?
Dr Piliang: In the clinical trials, the efficacy for eyebrows and eyelashes mirrored the efficacy for scalp hair. Somewhere between 25% and 45% of patients, depending on the drug and the dosage, regrew their eyebrows and eyelashes. It is incredibly important for patients to have access to these medications for eyebrows and eyelashes.
The Dermatologist: In your experience, how does the restoration of eyebrow and eyelash hair influence overall patient quality of life and treatment satisfaction?
Dr Piliang: I always look at eyebrows and eyelashes and document where we started and how much we have regrown. I do a lot of before and after photos of my patients, so we can use them to track their eyebrows and eyelashes. I think patients are very happy to have hair back, and they are especially happy to have eyebrows and eyelashes back because like I mentioned earlier, you can cover your scalp hair with a wig, but it is difficult to replicate eyebrows and eyelashes in a natural way. And they serve the functional purpose like we talked about also.
The Dermatologist: Are there any tips or insights you would like to share with your dermatology colleagues regarding the impact of eyebrow and eyelash loss in AA?
Dr Piliang: I would just emphasize that eyebrows and eyelashes are truly important for patients. They are important functionally to protect their eyes and they are also important for emotional and social well-being. Treating eyebrows and eyelashes is worthwhile and an essential aspect of care for patients with AA.