Wide-Rectus Abdominis Fascia Advancement: A Method for Treatment of Global Abdominal Wall Distention
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Background: Global abdominal wall distention (GAWD) is a phenomenon in which patients present with significant abdominal wall laxity and abdominal bulging unexplained by a rectus diastasis, large panniculus, or abdominal wall hernia. Traditional abdominoplasty techniques do not adequately address GAWD, and treatment of this condition requires modification of the abdominal fasciomuscular complex. This paper aims to describe a novel technique, known as wide-rectus abdominis fascia advancement (WRAFA), developed to address this vexing cosmetic issue.
Methods: Over a 30-year period, patients with GAWD were identified in a single surgeon's practice, and, once deemed to be appropriate candidates, they underwent the WRAFA procedure. All patients underwent the procedure in an outpatient setting and were kept for no longer than 23 hours or transferred to a certified recovery setting with skilled nursing. Aesthetic outcomes and complications were tracked over time.
Results: Six hundred eighty-five patients underwent abdominoplasty with the WRAFA technique. Two hundred eighty-four patients were available for follow-up for a minimum of 12 months. The average body mass index was 32. The median age was 38 years. Sex distribution was predominantly female (92.5% vs 7.75%). Aesthetic results were deemed to be good to excellent in 80% of patients, moderate in 15%, and minimal in 5%. None of the patients developed abdominal compartment syndrome. There were no fatalities or recurrences. One patient developed a unilateral lower quadrant hernia 15 years after the operation.
Conclusions: The WRAFA technique helps redefine the patient’s waistline while addressing functional muscular dystonia, ultimately providing excellent aesthetic and functional improvements.
Introduction
Global abdominal wall distention (GAWD) is a phenomenon of significant fascial laxity irreparable by traditional abdominoplasty, which does well in addressing diastasis recti but is not effective outside of the boundaries of the diastasis. GAWD is not well established in the literature, thus limiting the scientific criteria available. However, as a defined cosmetic issue, male and female patients alike present with a significant abdominal wall bulge that is not explained by the degree of rectus diastasis and/or the degree of thickness of the abdominal panniculus. Over time, even the well-established abdominoplasty may not adequately address the patient’s cosmetic concerns. Patients with GAWD may still have a protuberant abdominal wall without an aesthetically pleasing contour.
Diastasis recti abdominis (DRA) is defined as a longitudinal separation of the rectus abdominis muscles, leading to an anterior fascial bulge between the separated muscles. While DRA is well defined and treatable, GAWD is a different condition that involves the bulging of the entire abdominal wall. The exact etiology of this fascial laxity—and resultant abdominal bulging—is unknown and likely multifaceted. The literature indicates that, secondary to residual or recurrent diastasis recti, flaccidity of the muscular aponeurosis and/or baseline physiological incompetence are the major risk factors.1 Parity, age, prior caesarean section, significant alterations in weight, and concomitant hernia without documented repair are all issues that could contribute to abdominal wall distention.1,2 Various risk factors may contribute to the weakening of the abdominal wall’s fascial architecture, including postpartum status, irritable bowel syndrome (IBS), visceral fat, and lack of exercise. Interestingly, despite the emphasis placed on DRA as a cause of abdominal laxity, some patients do not have DRA; however, they present with significant GAWD. Others may have undergone DRA repair and still end up with residual and bothersome GAWD. Others do not have GAWD but have concomitant DRA and umbilical and paraumbilical hernias. Some may have all 3 conditions: DRA, GAWD, and hernias.
Abdominoplasty is a body contouring operation that helps address abdominal wall adiposity, skin laxity, and DRA. Various techniques, each with their own indications, are described in the literature today. The standard operation includes 3 key components: (1) removal of excess fat and skin, (2) vertical plication of the anterior rectus sheath, and (3) umbilical transposition.3,4 As mentioned, after an abdominoplasty and despite successful fascial plication, some patients fail to experience resolution of their GAWD.
This study proposes a new technique, termed wide-rectus abdominis fascia advancement (WRAFA), which effectively and safely treats GAWD with or without concomitant DRA. This technique involves recreation of a new linea alba by mobilizing the anterior rectus sheaths medial to the linea semilunaris and reapproximating them in the midline. This requires partition of the anterior rectus sheath in a fusiform shape at variable distances between the medial border of the rectus muscle and the linea semilunaris. In doing so, the abdominal wall surface area is significantly reduced, providing a redefined contour to the waistline and a flat contour to the anterior abdominal wall.
Materials and Methods
Over a 30-year period, patients with GAWD were identified in a single surgeon’s practice. Once identified as appropriate surgical candidates, they underwent an abdominoplasty that incorporated the wide-rectus abdominis fascia advancement (WRAFA) technique. Human subjects gave informed consent for the use of their images, and the study authors conformed to all appropriate institutional guidelines. All surgeries were performed in a certified office-based ambulatory surgical center, and patients were kept up to 23 hours in the surgical facility or transferred to a certified recovery house under qualified nursing care.
Perioperative management is critical to obtain successful results and have minimal complications. As soon as the first consultation is carried out, the patient is fit with an abdominal binder or shaper. The patient is instructed to wear the binder 24 hours a day, 7 days a week and perform breathing exercises. They are also instructed to gradually tighten the binder to the maximal level of tolerance. The maximum verified body mass index (BMI) to qualify for surgery is 35; if the patient has a BMI greater than 35, they are instructed to lose weight with diet and exercises. Some are referred for bariatric medical management and/or bariatric surgery.
Bowel preparation, like that used for gastrointestinal surgery, is routinely used prior to WRAFA surgery. Its use in abdominoplasty has been described in prior publication.5 This allows for deflation of the intestines, which facilitates closure of the abdominal wall. It will also decrease pressure on the vena cava and potentially decrease the risk of deep venous thrombosis (DVT) on the lower extremities.
The WRAFA technique involves raising the suprafascial abdominal flap while sparing the umbilical stalk, as in traditional abdominoplasty. Once the flaps have been raised, a bilateral longitudinal curvilinear incision is made in the anterior recti sheaths with the widest point at or slightly above the level of the umbilicus. This point is located over the medial, central, or lateral third of the rectus muscle, always medial to the linea semilunaris (Figure 1). Each curvilinear incision is then directed toward the xyphoid and pubic areas. The lateral borders of this incision are then medialized to create a new linea alba over the midline, thus imbricating the medial recti muscle posteriorly and pulling in-block the lateral recti, external and internal obliques, and transversus abdomini muscles medially. The original linea alba is automatically retracted posteriorly and the navel is deepened (Figures 2-7). A new, strong linea alba is created.
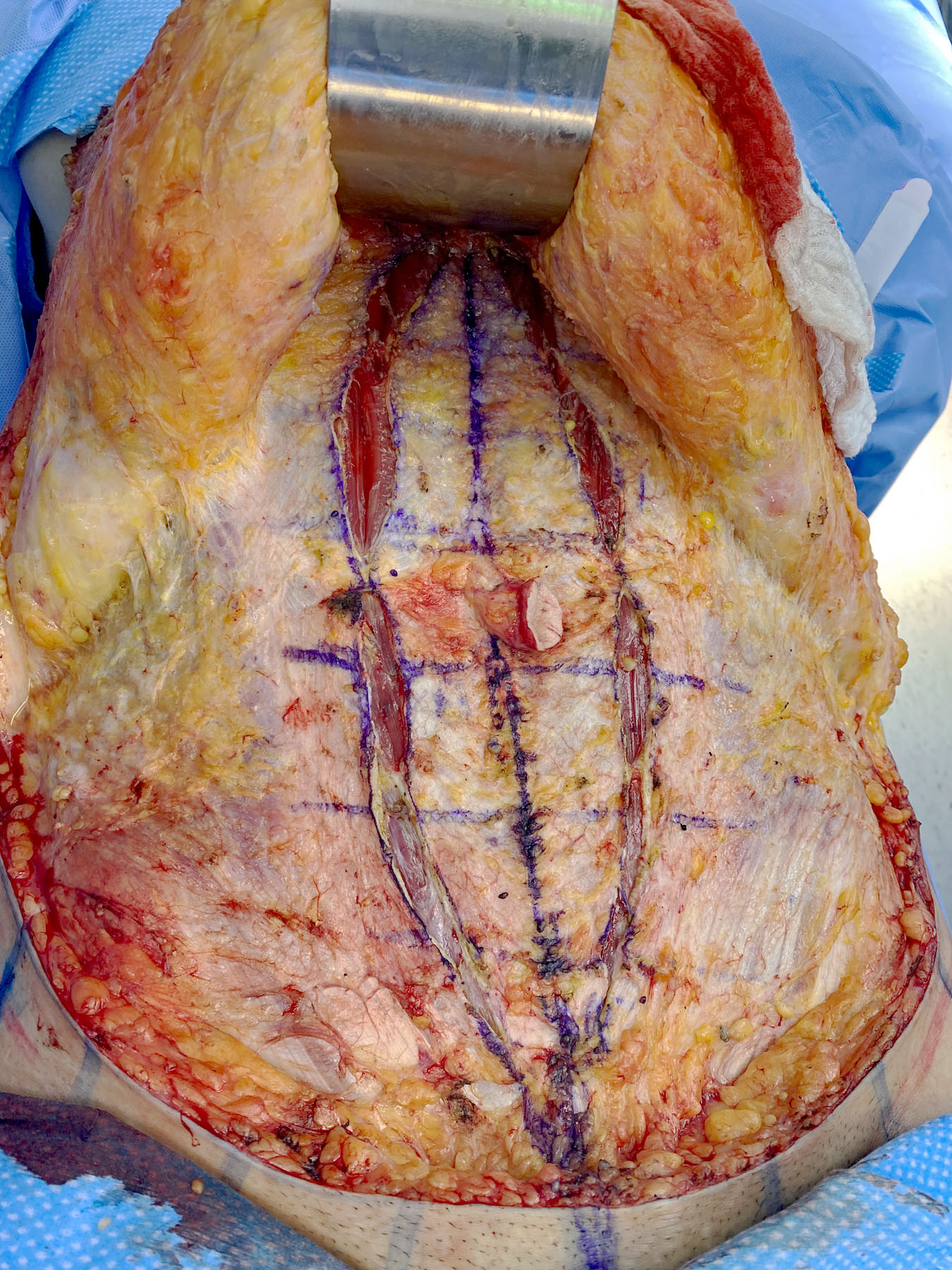
Figure 1. Incision of the anterior rectus sheath (rectus fascia partition) in a fusiform shape at variable distances between the medial border of the rectus muscle and the linea alba. The width around the umbilicus is 12 cm.
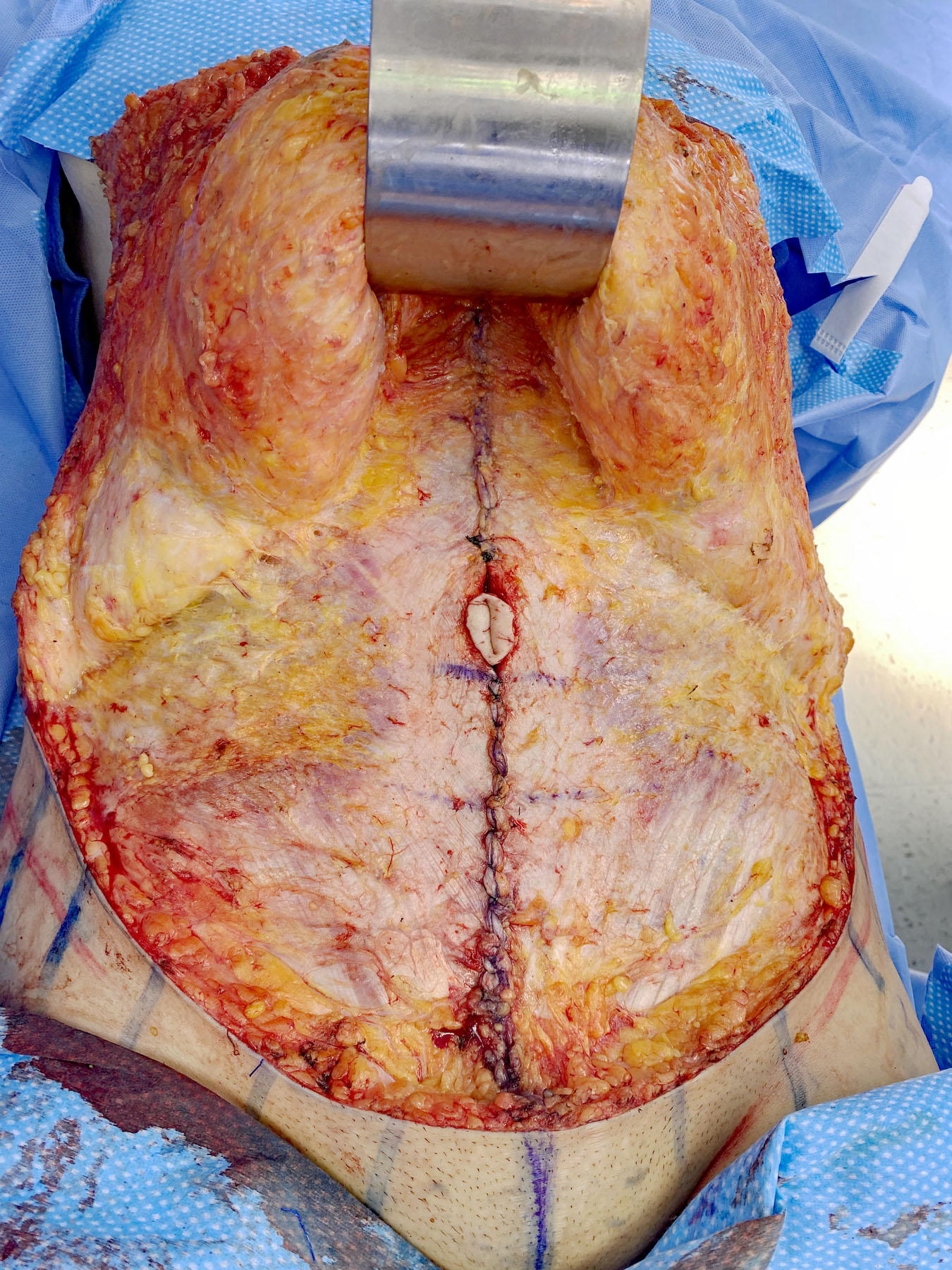
Figure 2. Image of the same surgical case as Figure 1 demonstrating the myofascial closure and creation of a new linea alba.
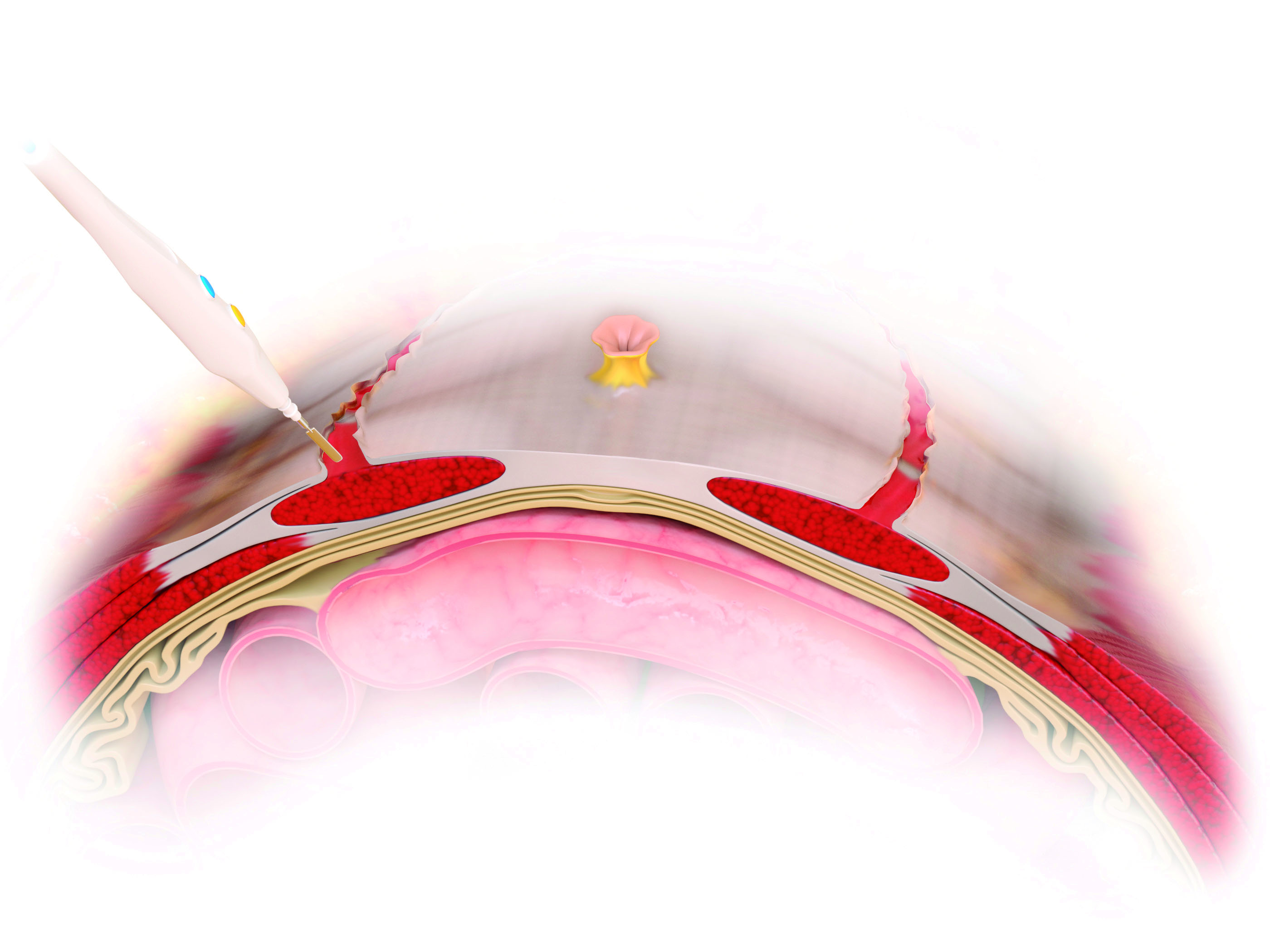
Figure 3. Tridimensional artistic view of the rectus fascia partition.
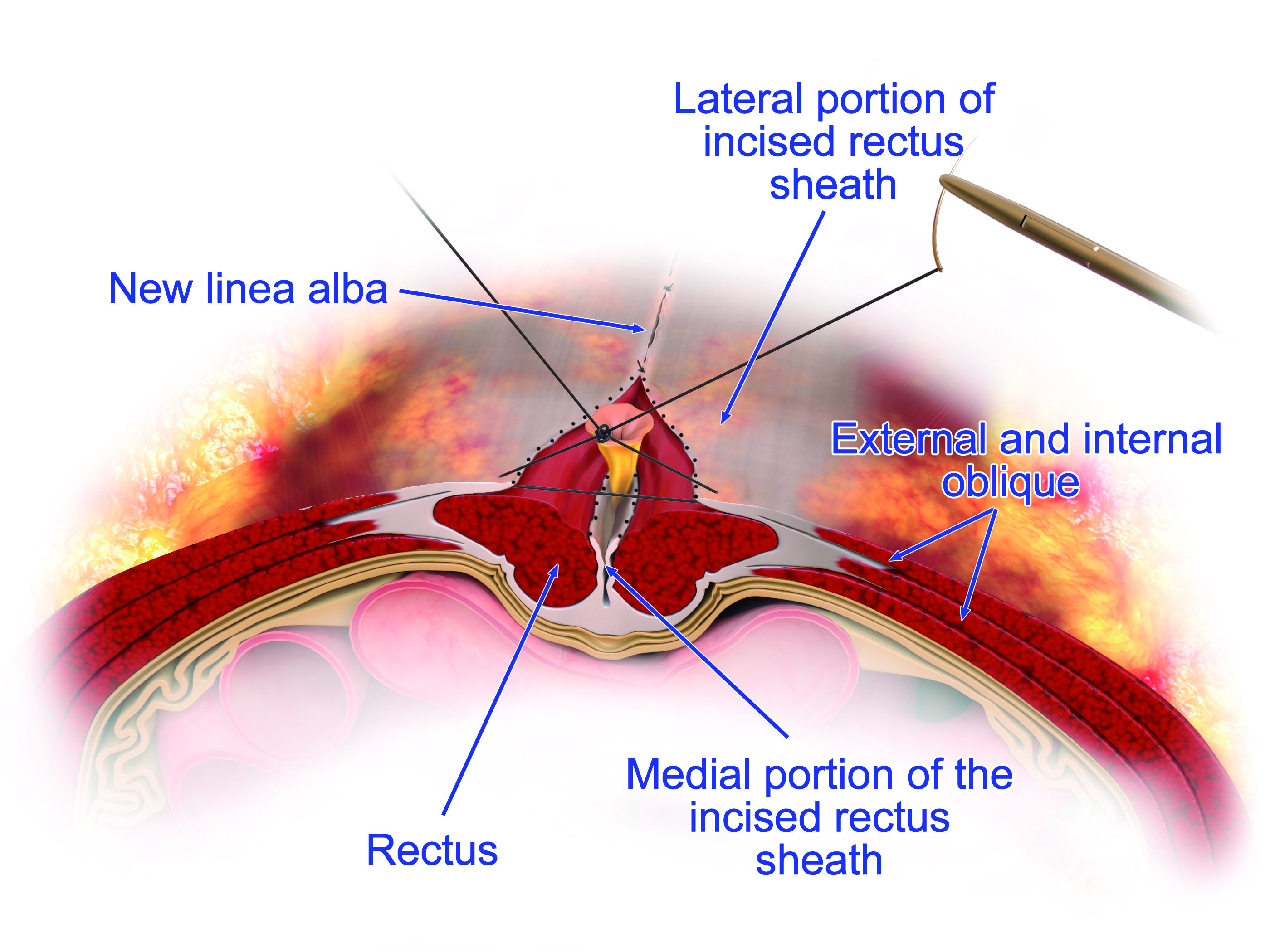
Figure 4. Tridimensional artistic view demonstrating closure at the midline and creation of the new linea alba from the external anatomic view, as well as the inversion of the myofascial edges with multiple interrupted sutures at the midline in the illustration.
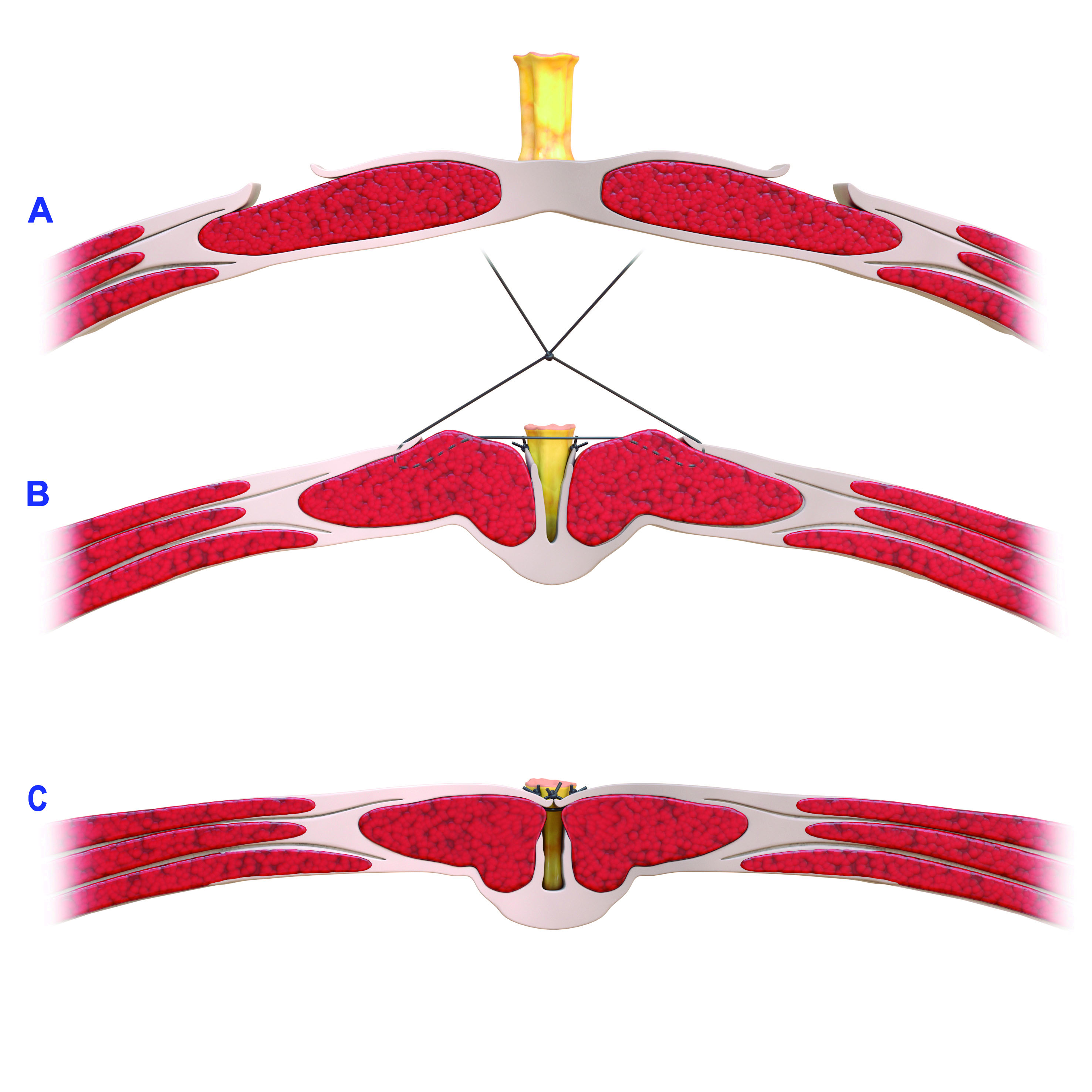
Figure 5. A-C. Wide-Rectus Abdominis Fascia Advancement from the axial view demonstrating recreation of a new linea alba via lateral anterior rectus sheath mobilization with re-approximation in the midline. Figure A demonstrates the native position of the lateral anterior rectus sheaths following incision. Figure B demonstrates medial mobilization of the anterior rectus sheaths medial to the linea semilunaris and reapproximating them in the midline, in order to create a new linea alba, as shown in Figure C.
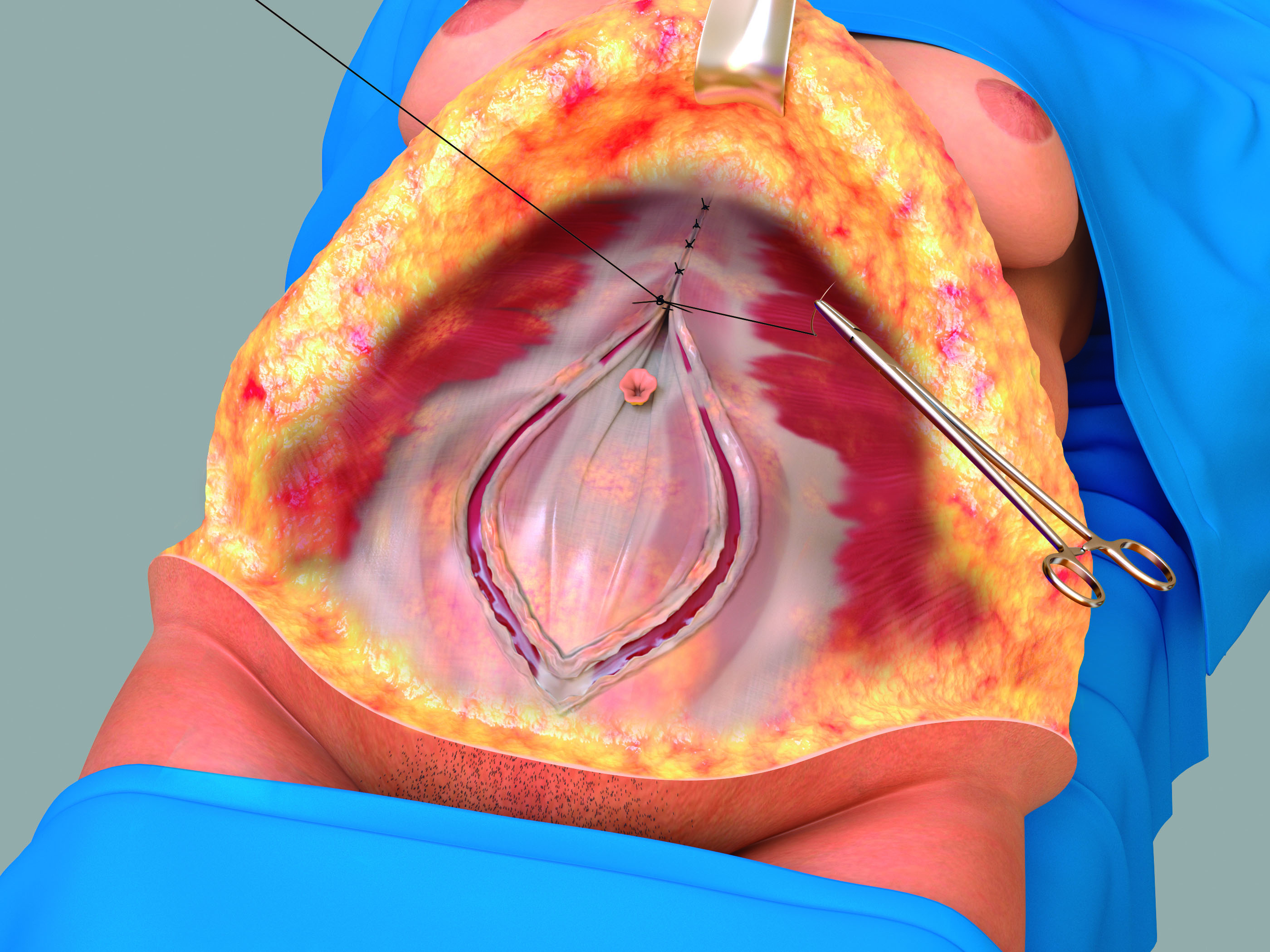
Figure 6. Artistic view of the creation of the new linea alba.
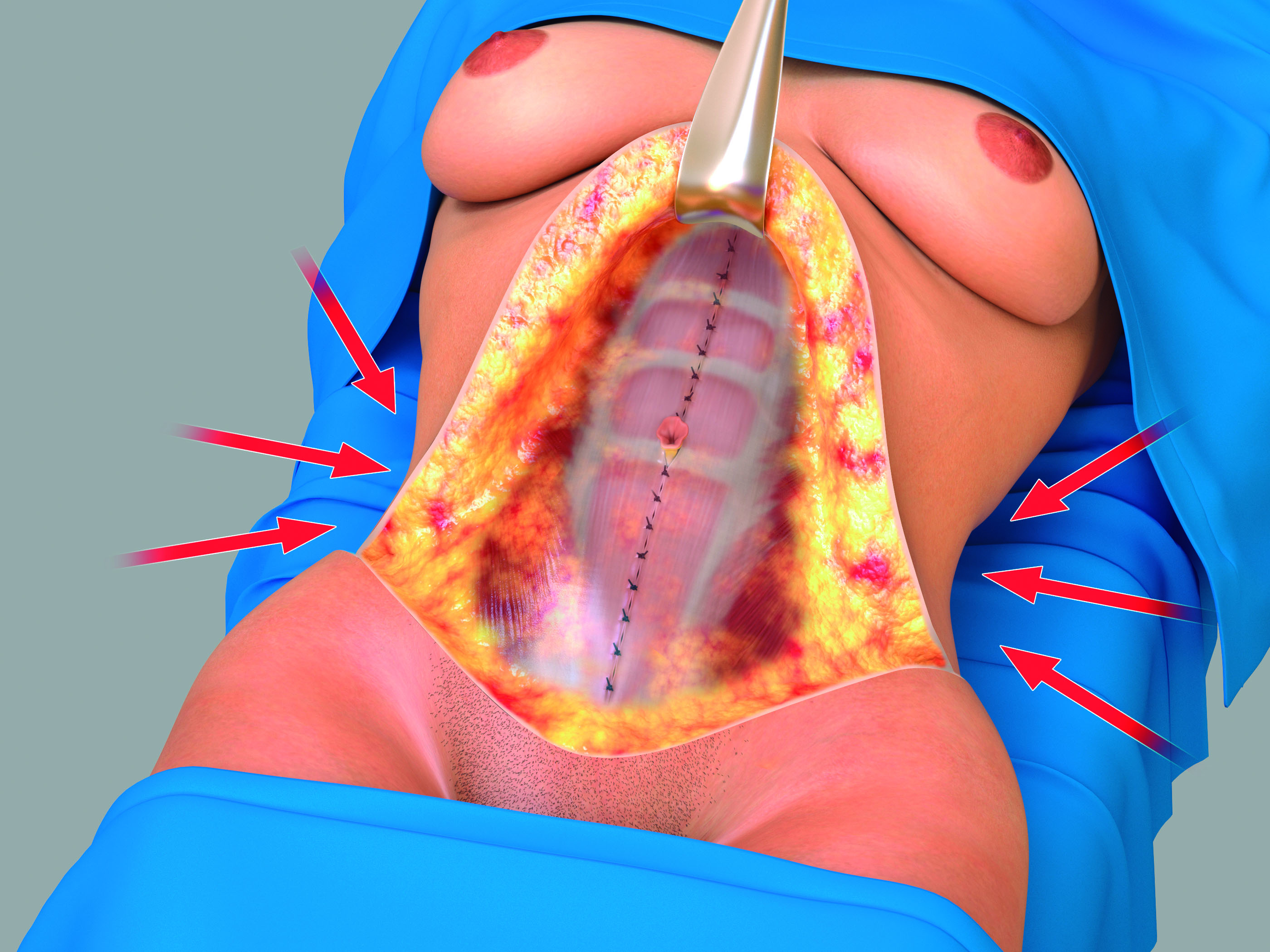
Figure 7. Demonstration of the dramatically improved contour of the waistline with the application of the Wide-Rectus Abdominis Fascia Advancement technique. This technique has also provided a flat contour to the anterior abdominal wall.
The WRAFA repair also addresses the defect in patients with concomitant DRA; no specific DRA repair is needed. However, patients with umbilical, periumbilical, or midline hernias require repair that involves opening the hernial sac and closing the peritoneal layer and overlying fascia. For these procedures, no biologic or alloplastic mesh is required. The WRAFA rectus imbrication will become another extra strong layer of repair.
By performing this medialization, myofascial laxity is addressed in both anterior and lateral aspects of the abdominal wall, effectively redefining the waistline and re-tensioning the abdominal muscles.
Results
From 1988 to 2022, 685 patients underwent abdominoplasty with the WRAFA technique to address GAWD. Patients with clear-cut symptoms of gas bloating, IBS, and other intestinal conditions were not included in this study and were referred for gastrointestinal treatment. Two hundred eighty-four patients were available for a follow-up for a minimum of 12 months. The average BMI was 32. The median age was 38 years. Sex distribution was predominantly female (92.5% vs 7.75%). Over 40% of the patients presented with neither a significant rectus diastasis (less than 4 cm) nor abdominal wall hernia; these patents can be categorized as pure GAWD. Around 20% presented with concomitant wide DRA (more than 5 cm), some of whom were diagnosed only intraoperatively because of the thick abdominal panniculus. Thirty percent of patients presented with umbilical and periumbilical hernias, some symptomatic and some without symptoms, and were only discovered during surgery. Around 25% of the patients had a combination of DRA and umbilical hernias. The range of horizontal dimensions of the approximation at their widest point was from 10 to 26 cm, with an average of 14.5 cm; these were measured without intravenous or other means of muscle relaxation. None of the patients developed abdominal compartment syndrome.
One patient had mucus aspiration with subsequent laryngeal spasm during extubation, leading to negative pressure pulmonary edema that required re-intubation and hospital admission for 48 hours. Her intraabdominal pressure was below the critical point of compartment syndrome despite a 26-cm width of the WRAFA incision and repair around the umbilicus. Because of the significant width of the defect to be repaired, an overlay of absorbable mesh (TIGR Matrix, Novus Scientific) was placed for extra support while healing (Video). She recovered uneventfully without disruption of the WRAFA repair. She was the only patient that developed DVT within the left femoral vein 10 days after her surgery despite mechanical and chemical DVT prophylactics. She was treated successfully with oral antiplatelet medication.
There were no fatalities, and none of the patients developed recurrence of GAWD. One patient developed a unilateral lower quadrant hernia 15 years after the operation.
Aesthetic results in the patients were deemed to be good to excellent in 80% of patients, moderate in 15%, and minimal in 5%. Cases 1-3 (Figures 8-23) demonstrate the dramatically improved body contour using the WRAFA technique. Of note, case 3 provides an example of the aesthetic advantages of this technique; however, in this case, the patient had an abdominoplasty 3 years prior with diastasis recti plication. This patient still had a larger residual GAWD, which highlights the cosmetic issue addressed with the WRAFA technique. Of note, the patient also underwent concomitant "owl" mastopexy,6 capsulectomy, and exchange of breast implants.
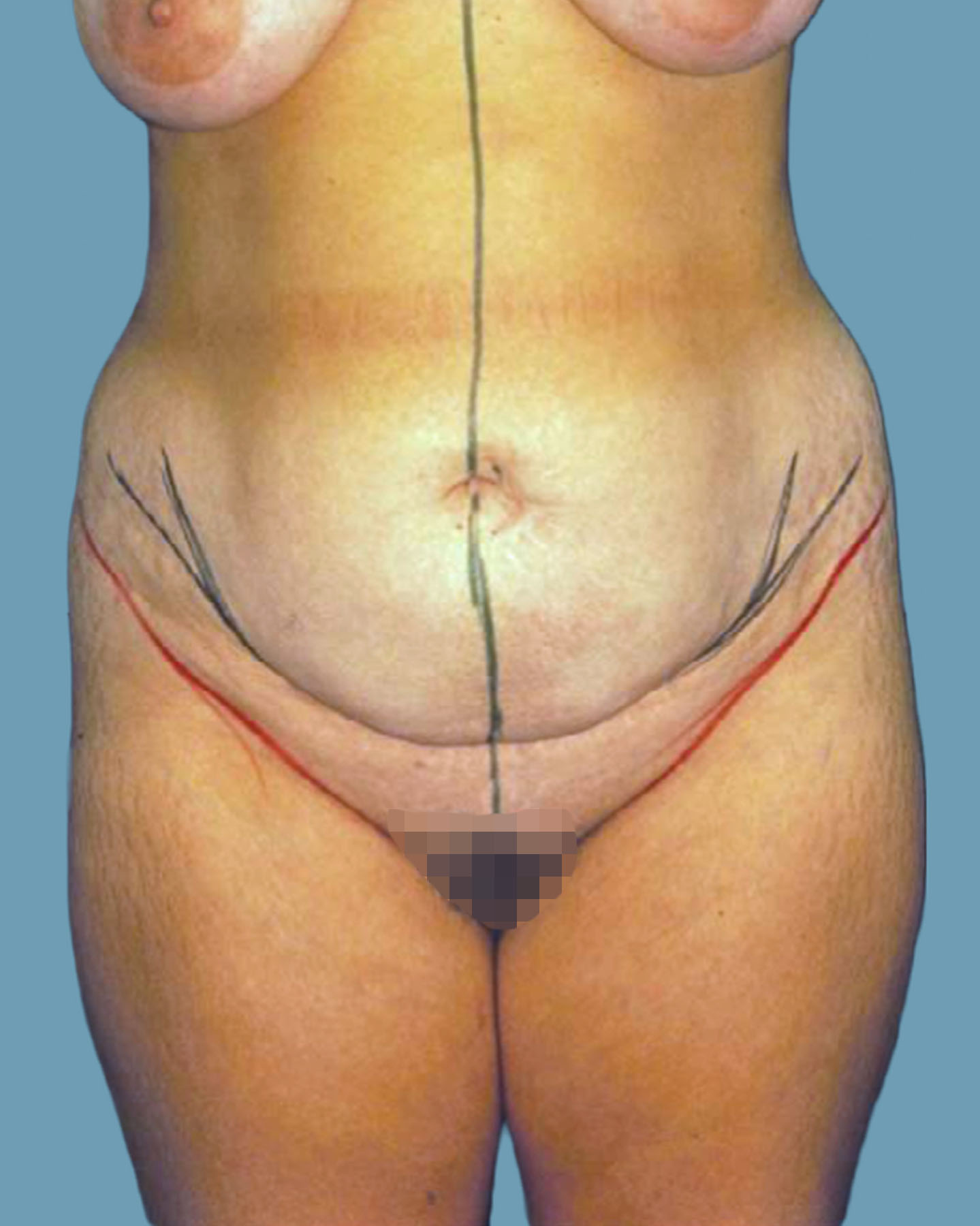
Figure 8. Case 1: A 22-year-old woman with history of twin pregnancy 2 years prior. The preoperative photo shows a wide waist, laxity, and protuberant bulging of the abdominal wall, typical of global abdominal wall distention. Her diastasis recti abdominis was relatively narrow (approximately 3-4 cm in width).

Figure 9. Case 1: Postoperative front view shows a reduced waistline and flattening of the abdominal wall.

Figure 10. Case 1: Preoperative lateral view shows the severity of the global abdominal wall distention and the increased lordosis.

Figure 11. Case 1: Postoperative lateral view shows improvement of the global abdominal wall distention with the wide-rectus abdominis fascia advancement technique. As an added functional benefit, the patient’s excessive lordosis has been corrected.

Figure 12. Case 2: Middle-aged man who exercised moderately. He presented with no midline abdominal or umbilical hernias. There was evidence of bulging abdominal wall.

Figure 13. Case 2: Postoperative front view shows improvement of contour with reduction of the global abdominal wall distention.

Figure 14. Case 2: Preoperative lateral view shows the global abdominal wall distention.
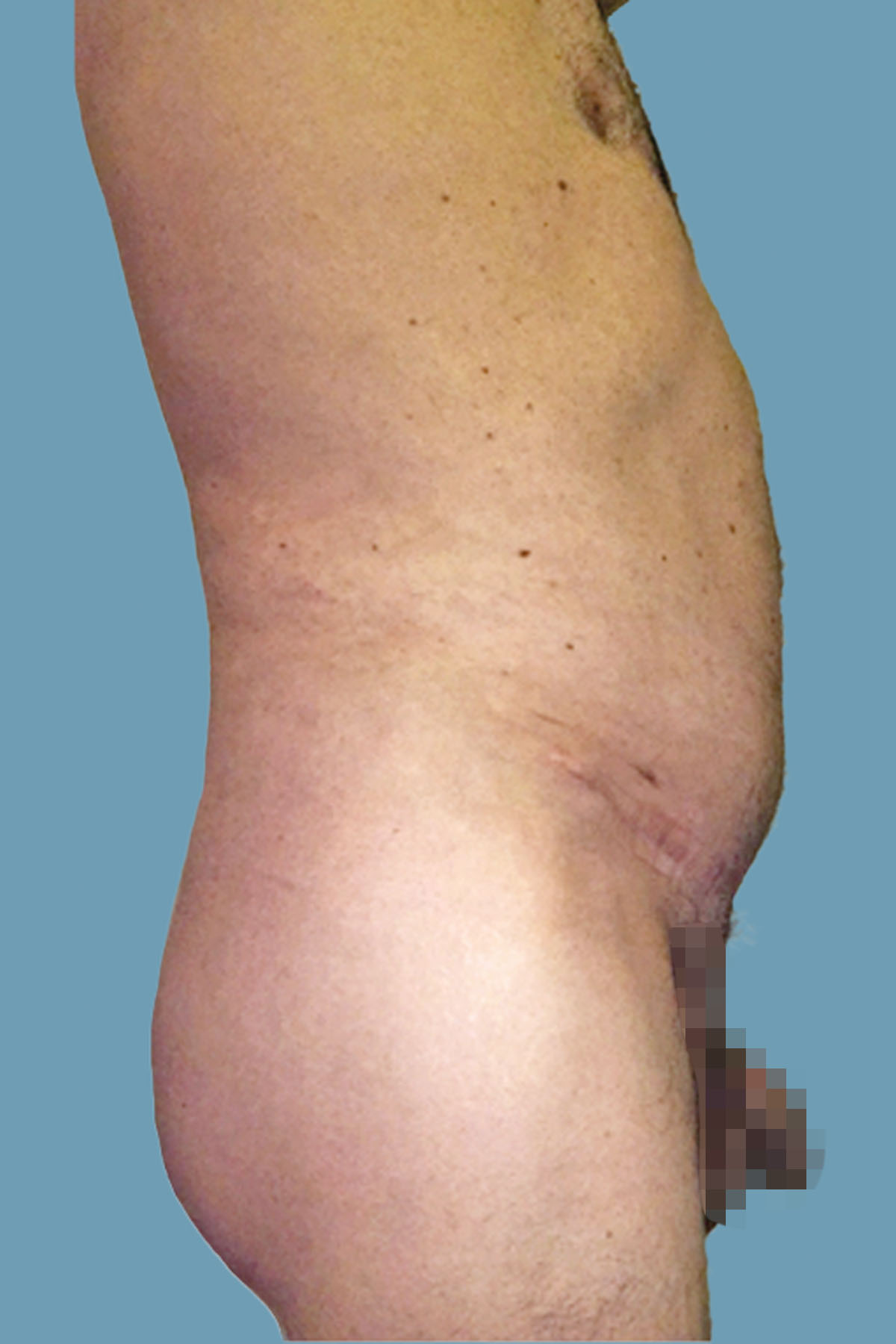
Figure 15. Case 2: Postoperative lateral view shows the significant clinical improvement in the abdominal wall protuberance. Comparative pre- and postoperative magnetic resonance imaging is shown in Figures 24 and 25.

Figure 16. Case 2: Preoperative view with a hip in flexion. Despite contraction of the abdominal muscles, the distention is unchanged.

Figure 17. Case 2: Postoperative view with a hip in flexion, with noticeable improvement.
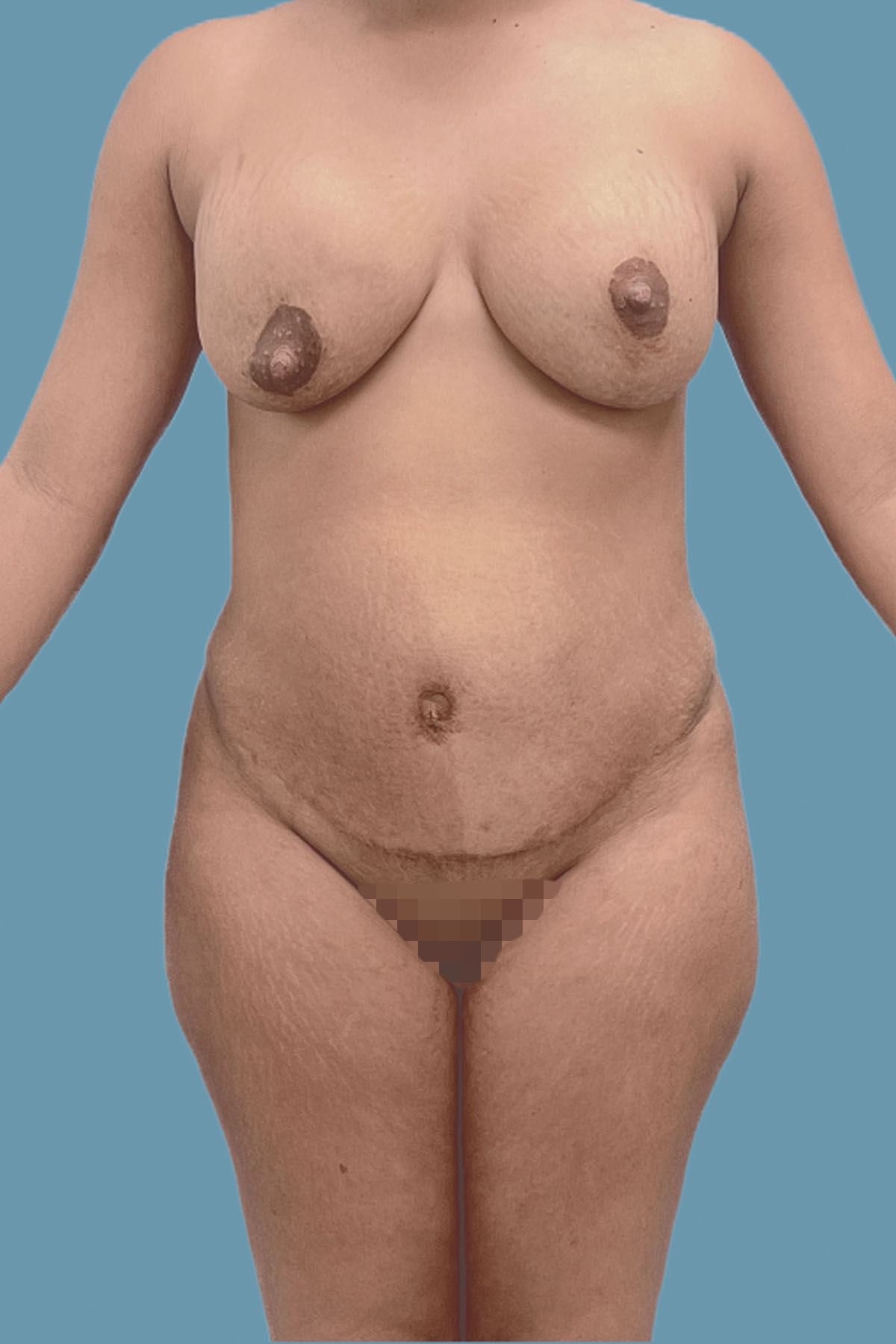
Figure 18. Case 3: Multiparous 28-year-old woman with a history of abdominoplasty with diastasis recti repair with plication 3 years prior. No recurrent diastasis recti abdominis; however, she presented with residual large global bulging of the abdominal wall.

Figure 19. Case 3: After extended abdominoplasty and wide-rectus abdominis fascia advancement repair, the abdomen is flat and waistline is improved. Patient also underwent concomitant "owl" mastopexy, capsulectomy, and exchange of breast implant exchange.

Figure 20. Case 3: Preoperative lateral view showing the obvious global abdominal wall distention.

Figure 21. Case 3: Postoperative lateral view, with noticeable flattening of the abdomen.

Figure 22. Case 3: Preoperative three-quarters view. Observe the global abdominal wall distention. The navel is flat and wide.

Figure 23. Case 3: Postoperative three-quarters view. The abdomen is flat; the navel is narrow and deep (“innie”). The body posture is also improved.
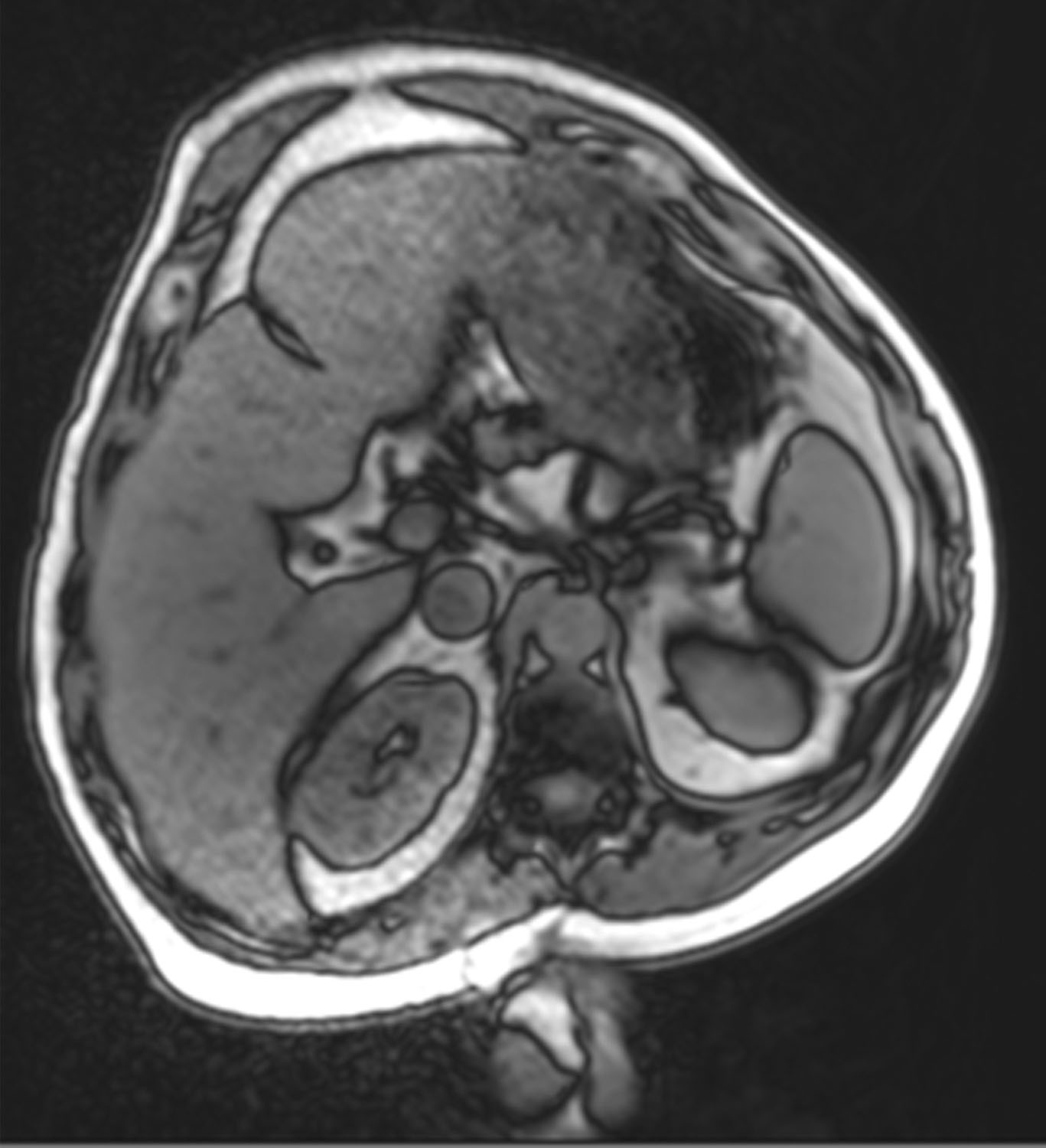
Figure 24. Case 2: Magnetic resonance imaging taken in left lateral decubitus. Note the dysmorphic protuberant anterior abdominal wall preoperatively.
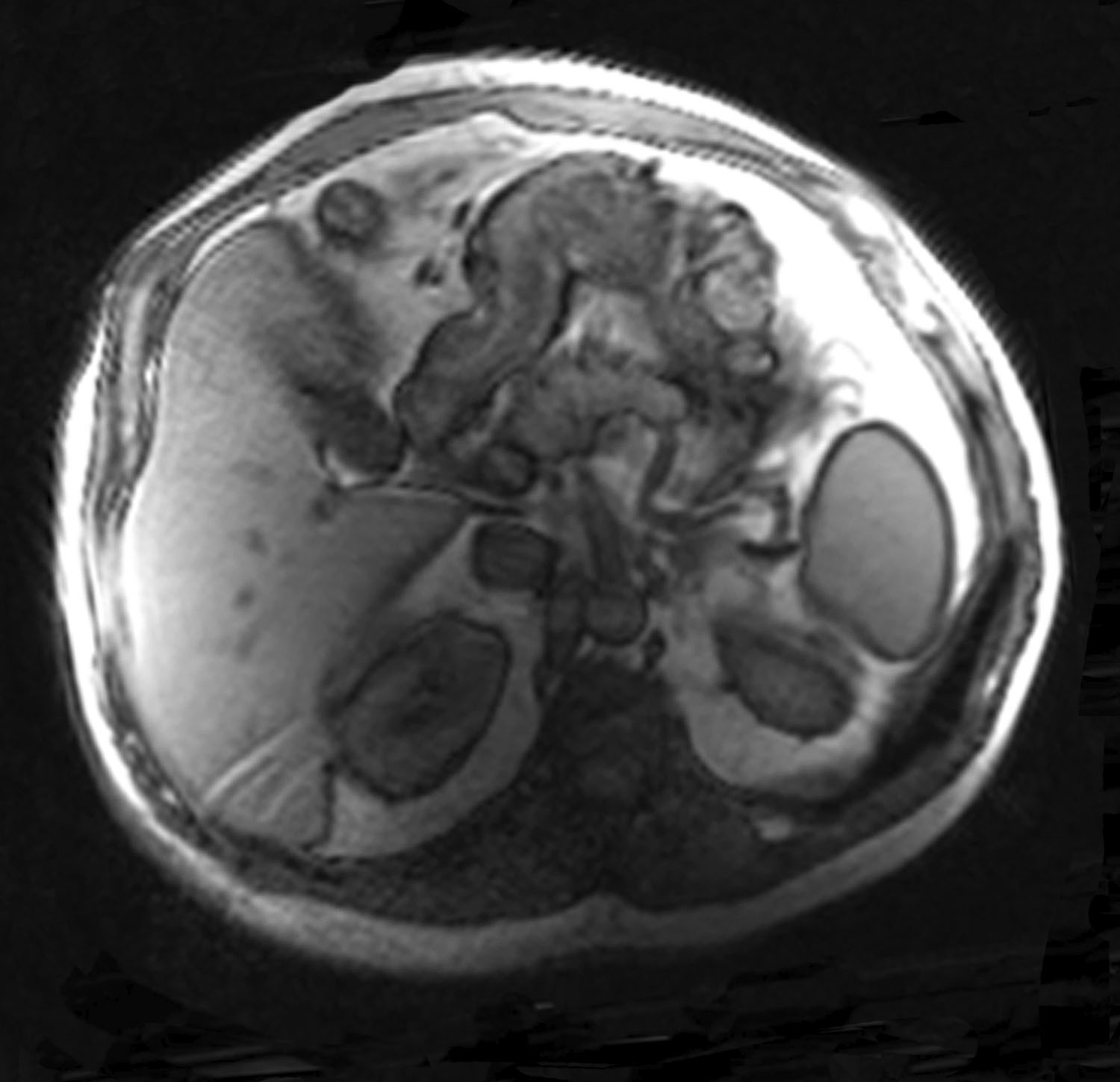
Figure 25. Case 2: Magnetic resonance imaging view shows the improved abdominal wall shape postoperatively along with the hypertrophied abdominal wall musculature.
Discussion
The abdominoplasty technique can vary from simple to complex depending on the patient’s condition and their desired functional and aesthetic goals. The WRAFA technique is meant to re-tension the distended abdominal wall musculature in GAWD to not only redefine the waistline but also correct any muscular dystonia caused by the distension, thus allowing for not only aesthetic refinement but also improved functional outcome.
Re-tensioning or improving abdominal wall laxity has multiple functional benefits to the patient. It has been shown that muscle displacement from anatomic position due to hernias or DRA can impair optimal muscle function.7 Criss et al showed that the reestablishment of rectus musculature in the normal anatomic position by recreating the linea alba through rectus medialization in patients with ventral hernias improved isokinetic and isometric measurements on postoperative dynamometer, as well as patient-reported quality of life.7 Similar displacement of the musculature occurs in patients affected by DRA, and there is some evidence to suggest that the reestablishment of normal muscular anatomy during plication of DRA has a similar effect by improving muscle strength;8 however, this claim is controversial in the literature.9
Although the rectus muscle location is not the primary component of the abdominal wall addressed though the WRAFA technique, similar functional benefits have been reported in the literature as a result of re-tensioning the oblique muscles through medialization. Recent work by O’Neal et al,10 based on the work by Toranto,11,12 showed that wide rectus abdominis plication was a viable option for the treatment of chronic intractable back pain. The mechanism of action is thought to be due to multiple reasons, all of which lead to increased spine stabilization. These include tightening of the lateral muscular complex, which leads to increased abdominal pressure, and thus places the musculature in a more efficient position in the force/length curve to allow for better force generation.10 These effects of improved spinal stabilization were objectively measured and confirmed by Temel et al through improvements in posture, lumbar lordosis, thoracic kyphosis, and lumbosacral angle in patients 6 months post-abdominoplasty with rectus plication.13
Conceptually, this technique is similar to the wide abdominal rectus plication (WARP) technique described by Toranto.11 However, the WRAFA technique incises the anterior rectus sheath for the repair instead of plicating it directly. The reasoning behind the incisions rather than direct plicating is based upon the concepts borrowed from component separation.14 Incising the anterior rectus sheath helps decrease the index of tension of the abdominal wall closure and the aponeurotic edges of the fascia and helps better redefine the waistline compared with direct plication.5,14-17 With the WRAFA technique, we contend that the oblique muscles are pulled medially more effectively than in traditional plication techniques. Using a "component separation" approach, we are able to better address a tense abdominal wall, potentially under increased intra-abdominal pressure, and more easily mobilize the rectus muscles. This helps accommodate intra-abdominal contents and address an otherwise bloated appearance, as seen in the included preoperative images (Figures 9, 14, and 20). This is especially true in patients with a very wide rectus diastasis. It also allows effective shortening and deepening of the long navel stalk.18
There is concern that such advancement of obliques may obscure the definition of the rectus abdominis in the anterior abdominal wall, thus leading to a lack of an athletic appearance of the abdomen.19 However, this concern has been unfounded in our patients. The rectus abdominis definition has remained prominent and visible in the postoperative patient. Ultimately, this technique may in fact be superior to other methods, including the standard rectus sheath plication, given the overall width of rectus sheath plication achieved with the WRAFA technique. By mobilizing the anterior rectus sheaths medial to the linea semiluminaris after partitioning them, the abdominal wall surface area can be reduced to a greater extent than other methods, thus providing a more desirable cosmetic outcome for patients with GAWD.
This technique involves recreation of a new linea alba by mobilizing the anterior rectus sheaths medial to the linea semilunaris and reapproximating them in the midline. As stated before, this requires partition of the anterior rectus sheath in a fusiform shape at variable distances from the medial rectus muscle and linea semilunaris. Thereby, the abdominal wall surface area is reduced, providing a narrower waistline and flatter contour to the anterior abdominal wall.
Furthermore, we have noted hypertrophy of the abdominal wall musculature after tightening, as is supported in postoperative magnetic resonance imaging scans, which have demonstrated hypertrophied muscle along with an improved overall abdominal wall shape because of globally restored muscular tension. In parallel, Hicks et al noted muscular hypertrophy after the creation of a new linea alba following abdominal component separation.20 We theorize that this phenomenon is likely due to repositioning the muscle in a better position on the force/length curve, as discussed above.
Limitations
This study is has multiple limitations, which include the inability to address all the potential underlying causes of GAWD. The cause of GAWD is likely multifaceted, similar to the causes of DRA. The cause could also be chronic distension of the anterior abdominal wall, which could be due to increased intra-abdominal visceral content or repetitive episodes of bloating caused by an abnormal muscular response to increasing intra-abdominal pressure, as described by Tremolaterra et al.21 If there is increased intra-abdominal content or repetitive functional bloating causing GAWD, this would not be addressed by WRAFA and may potentially lead to recurrence of GAWD in long-term follow-up, though longer follow-up of these patients would be required to elucidate recurrence rates. However, many patients were followed for several years, and the abdominal repair and shape has been maintained stable. It is feasible that the WRAFA repair produces significant changes to the abdominothoracic mechanisms, including the repositioning of the diaphragm, leading to more permanent and long-standing changes.22 Many of these patients have also made changes to their lifestyle, including increased physical activities and improvement of their diet with loss of weight and visceral fat. Overweight and obese patients presenting with increased visceral fat are key factors that contribute to GAWD. Improvement of GAWD in post-pregnancy patients is more straightforward to understand.
Another limitation is the single-center and single-surgeon design. However, we believe our study represents a significant portion of the population that presents with GAWD and have proposed a method to effectively manage the condition to allow for effective and reproducible outcomes without any significant procedure-related long-term morbidity. Though this study serves as an introduction to the technique and the possibilities it may yield for better aesthetic and functional outcomes for our patients, more investigation will be required to better define the condition and the ideal candidate to undergo WRAFA.
Conclusions
The WRAFA technique provides patients with a contoured waistline while simultaneously addressing GAWD. This study demonstrates that patients experience excellent cosmetic outcomes with few overall complications. This method should therefore be integrated into the plastic and reconstructive surgeon’s arsenal when considering ways to address abdominal laxity combined with bulging of the abdominal wall.
Acknowledgments
Authors: Oscar M. Ramirez, MD1; Munir Patel, MD1; Grant Schalet, MD1; Vitali Azouz, MD1; Marcio Yuri Ferreira, MD3
Affiliations: 1Division of Plastic and Reconstructive Surgery, Cleveland Clinic Florida, Weston, Florida; 2Department of Surgery, Broward Health Medical Center, Fort Lauderdale, Florida; 3Universidade Federal de Sao Paulo, Sao Paulo, Brazil
Correspondence: Grant Schalet, MD, Broward Health Medical Center, Graduate Medical Education, 1600 S. Andrews Avenue, Fort Lauderdale, FL 33316, USA. Email: gschalet@browardhealth.org
Presented as an Abstract at the American Association of Plastic Surgeons (AAPS) Centennial Meeting; April 9-12, 2022; San Diego, California.
Disclosures: Dr Ramirez is a consultant for Marina Medical LLC, consultant for Poriferous LLC, and consultant for Villani Spongilla Matrix.
References
- Caldeira AML, Carrión K, Jaulis J. Repair of the severe muscle aponeurotic abdominal laxity with alloplastic mesh in aesthetic abdominoplasty. Aesthetic Plast Surg. 2018;42(4):1039-1049. doi:10.1007/s00266-018-1101-6
- Lincenberg SM. The retro-rectus prosthesis for core myofascial restoration in cosmetic abdominoplasty. Aesthet Surg J. 2017;37(8):930-938. doi:10.1093/asj/sjx027
- Pitanguy I. Abdominal lipectomy: an approach to it through an analysis of 300 consecutive cases. Plast Reconstr Surg. 1967;40:384-394. doi:10.1097/00006534-196710000-00012
- Grazer FM. Abdominoplasty. Plast Reconstr Surg. 1973;51(6):617-623. doi:10.1097/00006534-197306000-00001
- Ramirez OM. Abdominoplasty and abdominal wall rehabilitation: a comprehensive approach: Plast Reconstr Surg. 2000;105(1):425-435. doi:10.1097/00006534-200001000-00069
- Ramirez OM. Reduction mammaplasty with the "owl" incision and no undermining. Plast Reconstr Surg. 2002;109(2):512-522; discussion 523-524. doi:10.1097/00006534-200202000-00016
- Criss CN, Petro CC, Krpata DM, et al. Functional abdominal wall reconstruction improves core physiology and quality-of-life. Surgery. 2014;156(1):176-182. doi:10.1016/j.surg.2014.04.01
- Olsson A, Kiwanuka O, Wilhelmsson S, Sandblom G, Stackelberg O. Cohort study of the effect of surgical repair of symptomatic diastasis recti abdominis on abdominal trunk function and quality of life. BJS Open. 2019;3(6):750-758. doi:10.1002/bjs5.50213
- Gormley J, Copeland A, Augustine H, Axelrod C, McRae M. Impact of rectus diastasis repair on abdominal strength and function: a systematic review. Cureus. 2020;12(12):e12358. doi:10.7759/cureus.12358
- Oneal RM, Mulka JP, Shapiro P, Hing D, Cavaliere C. Wide abdominal rectus plication abdominoplasty for the treatment of chronic intractable low back pain. Plast Reconstr Surg. 2011;127(1):225-231. doi:10.1097/PRS.0b013e3181fad2f7
- Toranto IR. The relief of low back pain with the WARP abdominoplasty: a preliminary report. Plast Reconstr Surg. 1990;85(4):545-555. doi:10.1097/00006534-199004000-00009
- Toranto IR. Resolution of back pain with the wide abdominal rectus plication abdominoplasty. Plast Reconstr Surg. 1988;81(5):777-779. doi:10.1097/00006534-198805000-00024
- Temel M, Türkmen A, Berberoğlu Ö. Improvements in vertebral-column angles and psychological metrics after abdominoplasty with rectus plication. Aesthet Surg J. 2016;36(5):577-587. doi:10.1093/asj/sjv257
- Ramirez OM, Ruas E, Dellon AL. "Components separation" method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86(3):519-526. doi:10.1097/00006534-199009000-00023
- Nahas FX, Ishida J, Gemperli R, Ferreira MC. Abdominal wall closure after selective aponeurotic incision and undermining. Ann Plast Surg. 1998;41(6):606-613; discussion 613-617. doi:10.1097/00000637-199812000-00005
- Barbosa MV, Ayaviri NA, Nahas FX, Juliano Y, Ferreira LM. Improving tension decrease in components separation technique. Hernia. 2014;18(1):123-129. doi:10.1007/s10029-013-1094-7
- Faustino LD, Ferreira LM, Ramirez OM, Nahas FX. Components separation technique of the abdominal wall: Which muscle release produces the greatest reduction in tension on the mideline? J Plast Reconstr Aesthet Surg. 2021;74(12):3361-3370. doi:10.1016/j.bjps.2021.05.015
- Ramirez, OM. Umbilical reconstruction with the “heart-shaped incision”. In: Schiffman MA, ed. Adult Umbilical Reconstruction. Springer, Cham; 2017:225-246. doi:10.1007/978-3-319-43887-0_24
- Yousif NJ, Lifchez SD, Nguyen HH. Transverse rectus sheath plication in abdominoplasty. Plast Reconstr Surg. 2004;114(3):778-784. doi:10.1097/01.prs.0000131023.09405.a
- Hicks CW, Krpata DM, Blatnik JA, Novitsky YW, Rosen MJ. Long-term effect on donor sites after components separation: a radiographic analysis. Plast Reconstr Surg. 2012;130(2):354-359. doi:10.1097/PRS.0b013e3182589d79
- Tremolaterra F, Villoria A, Azpiroz F, Serra J, Aguadé S, Malagelada JR. Impaired viscerosomatic reflexes and abdominal-wall dystony associated with bloating. Gastroenterology. 2006;130(4):1062-1068. doi:10.1053/j.gastro.2005.12.036
- Barba E, Burri E, Accarino A, et al. Abdominothoracic mechanisms of functional abdominal distension and correction by biofeedback. Gastroenterology. 2015;148(4):732-739. doi:10.1053/j.gastro.2014.12.006