


How I Treat: Complex Wound Closure

Sponsored
Aseptically Processed Human Allografts Use in Complex Wound Closure
Author Name
Frank Nastanski, MD, Orange County Global Medical Center, Santa Ana, CA
Patient Presentation
Case 1
- 58-year-old male
- Past medical history included hepatitis C as well as methamphetamine and heroin use
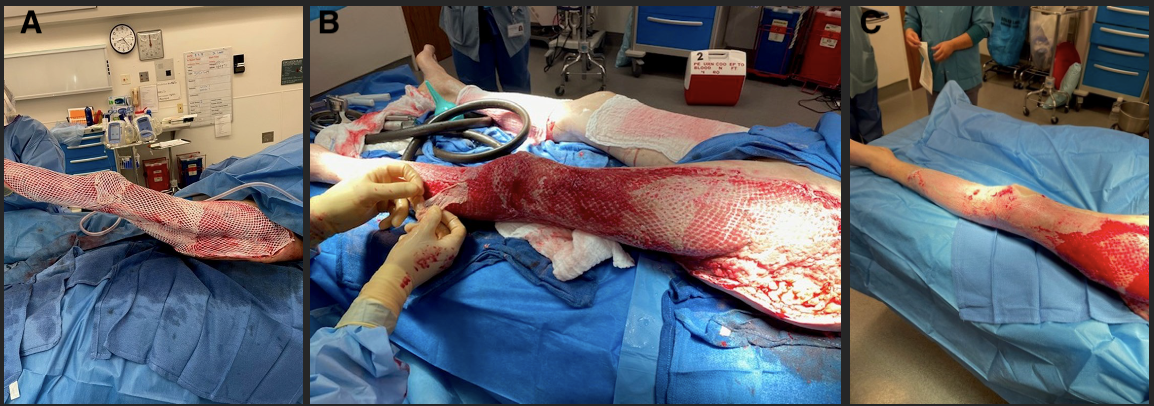
- The patient presented with a cut to his left knee from a fall while “urban camping” that had progressed to cellulitis in his entire leg with pus draining from the wound
- The infection affected the skin, muscle, fascia, joint capsule, and some areas of periosteum, which required aggressive serial debridement (Figure 1)

Case 2
- 41-year-old female
- Past medical history included morbid obesity and type 2 diabetes
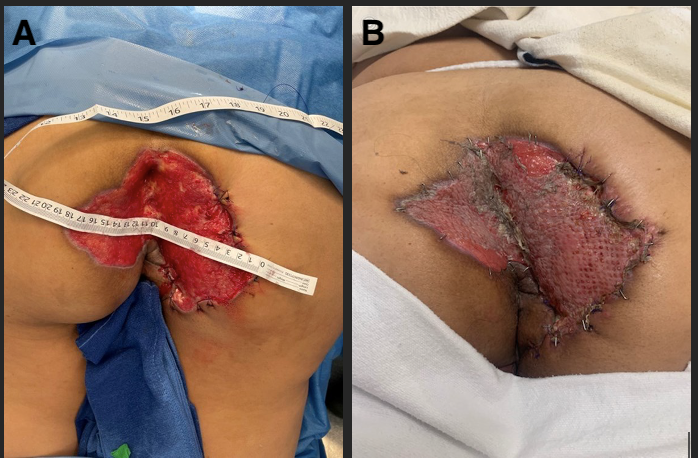
- The patient presented with an abscess to the buttocks that had progressed to necrotizing fasciitis of the perineum bilateral buttocks and sacrum, which required 2 rounds of debridement with IV antibiotic therapy (Figure 2)

Procedure and Treatment
Case 1
- After the infection was controlled, meshed human reticular acellular dermal matrix (HR-ADM) was secured to the wound bed using temporary surgical staples, and negative pressure wound therapy was applied
- After 10 days, the knee and lower leg received skin grafts, with autografting of the upper leg and hip 4 days later (Figure 3)
Case 2
- Once the infection was cleared, tunneling wounds of the right buttock and ischiorectal fossa were closed using soft tissue advancement flaps
- The dead space was filled using meshed HR-ADM, which was also utilized to maintain contour and avoid fluid collections
- Contour and bulk were created in the area by injecting allograft adipose matrix into the fatty tissues, and dehydrated amnion/chorion membrane was applied to the wound to support skin grafting (Figure 4)
Clinical Outcomes
Case 1
The wound was nearly closed and the knee had near normal range of motion within 6 weeks (Figure 5)

Case 2
The patient was fully continent of stool and flatus at 4 weeks (Figure 6)

