


Adapting CPR on Bariatric Patients
Scenario
It’s 2200 on a Friday night when the call comes out: “45-year-old male short of breath, cold and clammy.” Everyone yanks on their boots and jogs to the rigs but despite the purpose everyone moves with the call updates just as the first rig peels out of the garage: “Patient pulseless, not breathing, telephone CPR in progress.”
En route, the plan is discussed and roles are assigned. Initially, everyone will drag the patient onto a rigid surface if he is found on a bed or couch. After that: One will take over compressions from the wife, another will carry in and attach the monitor pads to the patient. Another EMT will carry in the oxygen kit and bag the patient, her partner will carry in and work suction. The ranking officer will keep time; the rookie will be second in line for compressions.
The mood of the crew is calm and purposeful. Between drills and daily life, they’ve done this hundreds of times.
When you all walk in, there’s a moment of hesitation: the patient weighs at least 500 pounds. His much smaller wife got him off the bed and onto the floor by some unknown means.
The initial compressor asks the wife to move aside and takes over for her.
The provider attaching the pads looks up at you. “So do I need to press the pads into his chest or something for the shock? Do you need to set the electricity higher or what?”
What does this patient’s weight change? What does your team need to do differently to succeed here?
CPR on the Obese
Great news: Almost nothing. Generally speaking, resuscitation is the same for the very obese as it is for anyone else in both technique and prioritization.1
Obese people are more likely to have an out-of-hospital cardiac arrest. However, in what’s referred to as the “obesity paradox” they are actually more likely to survive neuro intact than their normal weight counterparts. One theory for this is that most very overweight people have obstructive sleep apnea. Therefore, their body is better-conditioned and more tolerant of periods of hypoxia, which are inevitable in cardiac arrest.
Chest Compressions
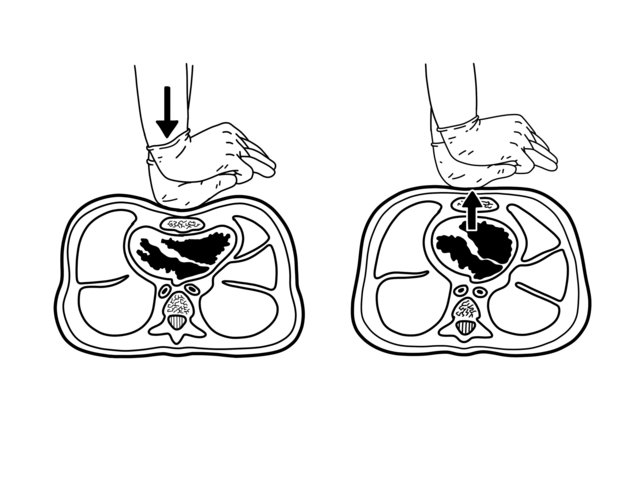
Chest compressions are the most important aspect of a good resuscitation.2 More than any amount of epinephrine given or breathing tubes placed in tracheas, the quality of the chest compression is the most important factor in determining whether or not this patient will be given a chance to survive. Good chest compressions also “prime the heart,” making it possible for the indicated shocks to work.
There are a few differences in the torso of very obese patients. The layer of tissue between the ribcage and the skin is thicker, and the chest cavity inside the ribcage is larger due to long-term changes in pressure gradients while breathing.
The recommended chest compression depth for normal-weight patients is 5 cm. This is probably not quite sufficient for very obese patients, due to both changes to their internal and external anatomy. However, the difference is only slight: you should aim for a compression depth of 6 cm for obese patients.
Ideally this will be accomplished with a direct, objective measurement like a CPR quality monitoring device.
Lacking that, press just a little deeper than usual and let the end-tidal CO2 reading be your guide. If it’s very low, try pressing a little deeper and recoiling more fully. Also, make sure to force even the strongest member of your crew to swap after two minutes. Objectively, these chest walls take more strength and energy to press down. Subjectively, first responders are universally reluctant to admit they’re exhausted.
In summary, chest compression on the very obese are almost identical to those on their normal weighted counterparts. They should be done 100 to 120 times a minute. Recoil is just as important as the press down, as the compression allows the brain to perfuse but the recoil perfuses the heart. Your patient really does need both of those organs.
Defibrillation
So how do we get electricity to these patient’s heart? We all know how important it is for a heart stuck in a dysrhythmia to be shocked effectively as quickly as possible. Won’t that shock be delayed, made less effective or even stopped completely in that layer of fat?
Though this concern makes complete logical sense, the answer is no.3
In 2017, a study tracked 574 patients who needed to wear an external AED as a stopgap until they could get a more definitive method to manage their heart problems. This device measured a lot of things, including both resistance to the shocks and their effectiveness. Over the study period, 624 shocks were administered collectively to the 574 people.
The device measured what’s known as “transthoracic impedence.” This is measured in Ohms and refers to the resistance the chest physically has to electricity running through it. As expected, heavier patients do have a higher transthoracic impedence. Patients with a normal BMI had one of about 44, while obese patients on average had one around 65. The study even recorded some very heavy individuals as having an impedance nearing 80.
That said, while the chest wall of these individuals was impeding the electricity, but the electricity worked anyway. The average first-shock success for normal-weight patients was 92.9%, and perhaps surprisingly, the average first-shock success for much heavier people was a percentage point higher, at 93.9%.
100 J is considered a sufficient shock for an average-weighted person. But we go up to 200 J, because it does no harm and just to make sure. This data suggests that 200 J will get through any chest wall effectively.
In conclusion, defibrillate and cardiovert the very obese precisely the same as you would anyone else. It’s actually a little more likely to work.
Conclusion
“No, just put the pads on like normal. And the Joule settings are the same that they always are.” Your mild tone and confident demeanor while you answer this question calms the entire crew and they return to their tasks.
You find your patient is in ventricular fibrillation. Compressions have already been going for a full minute so you shock him at 200J.
You get access via an IO drill while an EMT places a supraglottic airway. Another crew shows up and you assign one of them to monitor femorals and the second one to get in the compression line, being especially careful to make sure they’re switching every round.
At the next rhythm chest, the provider monitoring femorals announces that you all have a pulse. You start the ROSC timer and take a blood pressure: a totally respectable 160.
“Put the CPR machine on if it’ll go over his chest,” You instruct and the officer nods and runs to retrieve it.4
His wife touches your shoulder while your crew packs up the patient. “Is my husband going to be okay?”
You make very deliberate eye contact with the woman and offer the little comfort that can be given with integrity. “It’s possible. No matter what happens now, I need you to know that you’re the only reason we even made it this far. You did perfect. No one could have done more or better. Not even one of us.”
Works Cited
- Di Giacinto, I., Guarnera, M., Esposito, C., Falcetta, S., Cortese, G., Pascarella, G., Sorbello, M., & Cataldo, R. (2021). Emergencies in obese patients: a narrative review. Journal of anesthesia, analgesia and critical care, 1(1), 13. https://doi.org/10.1186/s44158-021-00019-2
- Lee, H., Oh, J., Lee, J., Kang, H., Lim, T. H., Ko, B. S., Cho, Y., & Song, S. Y. (2019). Retrospective study using computed tomography to compare sufficient chest compression depth for cardiopulmonary resuscitation in obese patients. Journal of the American Heart Association, 8(23). https://doi.org/10.1161/jaha.119.013948
- Wan, C., Szymkiewicz, S. J., & Klein, H. U. (2017). The impact of body mass index on the wearable cardioverter defibrillator shock efficacy and patient wear time. American Heart Journal, 186, 111–117. https://doi.org/10.1016/j.ahj.2017.01.007
- Lucas® 3, v3.1. Stryker. (2018). https://www.stryker.com/content/dam/stryker/ems/products/lucas-3/ca/FRENCH-CA_LUCAS3-v3.1_Brochure.pdf









